

SUBSCRIBE TO OUR FREE NEWSLETTER
Daily news & progressive opinion—funded by the people, not the corporations—delivered straight to your inbox.
5
#000000
#FFFFFF
To donate by check, phone, or other method, see our More Ways to Give page.
Daily news & progressive opinion—funded by the people, not the corporations—delivered straight to your inbox.
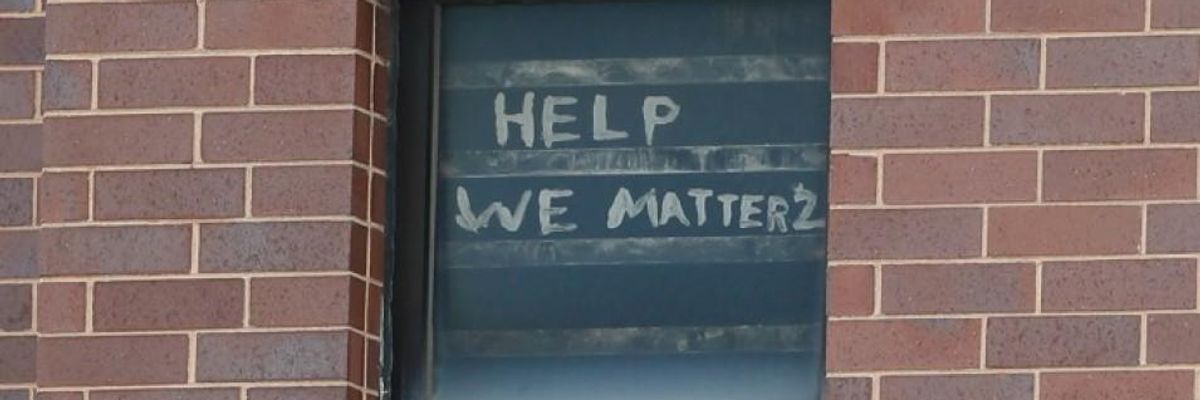
The words "help we matter 2" are seen written in a window at the Cook County Department of Corrections (CCDOC), housing one of the nation's largest jails, is seen in Chicago, on April 9, 2020. (Photo: Kamil Krzaczynski/AFP via Getty Images)
As the coronavirus pandemic continues to sweep through the country, especially in prisons and jails, the opioid epidemic has also seen a resurgence. The Washington Post reported that suspected overdoses jumped nationally by 18% in March, 29% in April, and 42% in May. This fits a nationwide pattern of excess deaths--deaths above the typical number anticipated by the CDC--unrelated to coronavirus, such as the increased toll from heart attacks, strokes, and cancer, all as our medical infrastructure is pushed to its limits.
There has never been a more critical time to provide medication for addiction treatment (MAT) for people with opioid use disorder (OUD).
There has never been a more critical time to provide medication for addiction treatment (MAT) for people with opioid use disorder (OUD). MAT consists of three FDA-approved medications--methadone, buprenorphine, and naltrexone--that treat OUD, the disease at the root of opioid addiction. MAT is basic healthcare and a cornerstone of care for tens of thousands of people in our communities who have OUD.
The need for MAT is particularly strong in jails and prisons: Without access to their medication, recently incarcerated people are left with few tools to battle their addiction. If provided with MAT, they are 74% less likely than people who are deprived of MAT to die of any cause while they are still incarcerated, and 85% less likely than people who are deprived of MAT to die of an overdose in the weeks after their release. Yet in the face of these stark numbers, 98% of jails and prisons still deny this lifesaving treatment to incarcerated people.
The small but growing number of prisons and jails that have implemented programs to provide MAT to incarcerated people with OUD have seen success. One study of the Rhode Island prison system, which was among the first to implement a robust MAT program, found that providing MAT reduced post-release deaths by 60%, and all opioid related deaths in the entire state by 12%. Sheriff Chris Donelan in Franklin County, Massachusetts reported a reduction in recidivism, overdose deaths, disciplinary concerns, and contraband after providing access to MAT.
In addition to saving lives, courts have found that providing MAT is a constitutional and civil right for incarcerated people. The Eighth Amendment to the U.S. Constitution bans "cruel and unusual punishment," which the Supreme Court has interpreted as prohibiting "deliberate indifference to serious medical needs." Further, the Americans with Disabilities Act (ADA) prohibits discrimination in public services, such as healthcare in jails, based upon a recognized disability, like OUD.
Last year, the First Circuit affirmed a ruling in the District of Maine under the ADA that a jail could not deny a woman serving a 40-day sentence access to the MAT prescribed to her by a doctor. This followed a decision by the District of Massachusetts that required a jail to provide an incarcerated individual with his prescribed MAT dose throughout his time in custody, holding that the denial of his medically necessary MAT was likely cruel and unusual punishment in violation of the Eighth Amendment as well as unlawful disability discrimination under the ADA.
As of July 22, more than 100,000 incarcerated people have been infected with Covid-19 and more than 760 have died. Even in the best of times, incarcerated people often receive substandard medical care, or no care at all. As Covid-19 cases make a resurgence in parts of the U.S. and continue to dramatically spike in jails, prisons, and detention facilities across the country, it has never been more important to provide evidence-based care for people with opioid use disorder in order to conserve hospital resources and save lives.
Our prisons and jails aren't designed to be drug rehab centers, and we must stop using them as such.
Our prisons and jails aren't designed to be drug rehab centers, and we must stop using them as such. Keeping people out of jail in the first place by making sure that they have reliable access to MAT both inside jails and prisons, and when they are out in the community, will help stop the rampant spread of Covid-19 and reduce the burden on our medical system.
Further, as researchers have pointed out, the symptoms of opioid withdrawal and Covid-19 can overlap. Without access to MAT for OUD, there is an increased danger that prison officials will miss suspected cases of Covid-19, assuming that the symptoms exhibited are a result of opioid withdrawal, when in fact they are symptoms of Covid-19. This creates a danger that a positive Covid-19 case could be missed by a correctional facility, allowing a positive individual to spread the disease to others with whom they share close quarters. The answer to this problem should never be solitary confinement.
Denying incarcerated people access to MAT adds a strain on the American healthcare system, even in the best of times. Nearly one quarter of America's prison and jail population of 2.2 million have OUD. During this crisis, it is even more imperative that people with OUD get access to the MAT they need. Instead of letting unlawful and scientifically unsound jail policies fill our hospital beds with people experiencing post-release overdoses, let's provide MAT to incarcerated people and use our hospitals to fight the Covid-19 crisis at hand.
We've already seen the federal government take some positive steps once thought impossible. This includes letting MAT patients take home their buprenorphine for 28 days in order to limit social contact while maintaining MAT treatment. While the federal Bureau of Prisons (BOP) has taken steps to expand access to MAT, the Department of Justice has supported recommendations from the Government Accountability Office aimed at making BOP improve the implementation of its MAT program so that it can serve everyone in need. It is time for Congress and state legislatures around the country to follow the lead of states like Rhode Island, and require MAT in all jails and prisons for everyone it is clinically appropriate for.
Dear Common Dreams reader, It’s been nearly 30 years since I co-founded Common Dreams with my late wife, Lina Newhouser. We had the radical notion that journalism should serve the public good, not corporate profits. It was clear to us from the outset what it would take to build such a project. No paid advertisements. No corporate sponsors. No millionaire publisher telling us what to think or do. Many people said we wouldn't last a year, but we proved those doubters wrong. Together with a tremendous team of journalists and dedicated staff, we built an independent media outlet free from the constraints of profits and corporate control. Our mission has always been simple: To inform. To inspire. To ignite change for the common good. Building Common Dreams was not easy. Our survival was never guaranteed. When you take on the most powerful forces—Wall Street greed, fossil fuel industry destruction, Big Tech lobbyists, and uber-rich oligarchs who have spent billions upon billions rigging the economy and democracy in their favor—the only bulwark you have is supporters who believe in your work. But here’s the urgent message from me today. It's never been this bad out there. And it's never been this hard to keep us going. At the very moment Common Dreams is most needed, the threats we face are intensifying. We need your support now more than ever. We don't accept corporate advertising and never will. We don't have a paywall because we don't think people should be blocked from critical news based on their ability to pay. Everything we do is funded by the donations of readers like you. When everyone does the little they can afford, we are strong. But if that support retreats or dries up, so do we. Will you donate now to make sure Common Dreams not only survives but thrives? —Craig Brown, Co-founder |
As the coronavirus pandemic continues to sweep through the country, especially in prisons and jails, the opioid epidemic has also seen a resurgence. The Washington Post reported that suspected overdoses jumped nationally by 18% in March, 29% in April, and 42% in May. This fits a nationwide pattern of excess deaths--deaths above the typical number anticipated by the CDC--unrelated to coronavirus, such as the increased toll from heart attacks, strokes, and cancer, all as our medical infrastructure is pushed to its limits.
There has never been a more critical time to provide medication for addiction treatment (MAT) for people with opioid use disorder (OUD).
There has never been a more critical time to provide medication for addiction treatment (MAT) for people with opioid use disorder (OUD). MAT consists of three FDA-approved medications--methadone, buprenorphine, and naltrexone--that treat OUD, the disease at the root of opioid addiction. MAT is basic healthcare and a cornerstone of care for tens of thousands of people in our communities who have OUD.
The need for MAT is particularly strong in jails and prisons: Without access to their medication, recently incarcerated people are left with few tools to battle their addiction. If provided with MAT, they are 74% less likely than people who are deprived of MAT to die of any cause while they are still incarcerated, and 85% less likely than people who are deprived of MAT to die of an overdose in the weeks after their release. Yet in the face of these stark numbers, 98% of jails and prisons still deny this lifesaving treatment to incarcerated people.
The small but growing number of prisons and jails that have implemented programs to provide MAT to incarcerated people with OUD have seen success. One study of the Rhode Island prison system, which was among the first to implement a robust MAT program, found that providing MAT reduced post-release deaths by 60%, and all opioid related deaths in the entire state by 12%. Sheriff Chris Donelan in Franklin County, Massachusetts reported a reduction in recidivism, overdose deaths, disciplinary concerns, and contraband after providing access to MAT.
In addition to saving lives, courts have found that providing MAT is a constitutional and civil right for incarcerated people. The Eighth Amendment to the U.S. Constitution bans "cruel and unusual punishment," which the Supreme Court has interpreted as prohibiting "deliberate indifference to serious medical needs." Further, the Americans with Disabilities Act (ADA) prohibits discrimination in public services, such as healthcare in jails, based upon a recognized disability, like OUD.
Last year, the First Circuit affirmed a ruling in the District of Maine under the ADA that a jail could not deny a woman serving a 40-day sentence access to the MAT prescribed to her by a doctor. This followed a decision by the District of Massachusetts that required a jail to provide an incarcerated individual with his prescribed MAT dose throughout his time in custody, holding that the denial of his medically necessary MAT was likely cruel and unusual punishment in violation of the Eighth Amendment as well as unlawful disability discrimination under the ADA.
As of July 22, more than 100,000 incarcerated people have been infected with Covid-19 and more than 760 have died. Even in the best of times, incarcerated people often receive substandard medical care, or no care at all. As Covid-19 cases make a resurgence in parts of the U.S. and continue to dramatically spike in jails, prisons, and detention facilities across the country, it has never been more important to provide evidence-based care for people with opioid use disorder in order to conserve hospital resources and save lives.
Our prisons and jails aren't designed to be drug rehab centers, and we must stop using them as such.
Our prisons and jails aren't designed to be drug rehab centers, and we must stop using them as such. Keeping people out of jail in the first place by making sure that they have reliable access to MAT both inside jails and prisons, and when they are out in the community, will help stop the rampant spread of Covid-19 and reduce the burden on our medical system.
Further, as researchers have pointed out, the symptoms of opioid withdrawal and Covid-19 can overlap. Without access to MAT for OUD, there is an increased danger that prison officials will miss suspected cases of Covid-19, assuming that the symptoms exhibited are a result of opioid withdrawal, when in fact they are symptoms of Covid-19. This creates a danger that a positive Covid-19 case could be missed by a correctional facility, allowing a positive individual to spread the disease to others with whom they share close quarters. The answer to this problem should never be solitary confinement.
Denying incarcerated people access to MAT adds a strain on the American healthcare system, even in the best of times. Nearly one quarter of America's prison and jail population of 2.2 million have OUD. During this crisis, it is even more imperative that people with OUD get access to the MAT they need. Instead of letting unlawful and scientifically unsound jail policies fill our hospital beds with people experiencing post-release overdoses, let's provide MAT to incarcerated people and use our hospitals to fight the Covid-19 crisis at hand.
We've already seen the federal government take some positive steps once thought impossible. This includes letting MAT patients take home their buprenorphine for 28 days in order to limit social contact while maintaining MAT treatment. While the federal Bureau of Prisons (BOP) has taken steps to expand access to MAT, the Department of Justice has supported recommendations from the Government Accountability Office aimed at making BOP improve the implementation of its MAT program so that it can serve everyone in need. It is time for Congress and state legislatures around the country to follow the lead of states like Rhode Island, and require MAT in all jails and prisons for everyone it is clinically appropriate for.
As the coronavirus pandemic continues to sweep through the country, especially in prisons and jails, the opioid epidemic has also seen a resurgence. The Washington Post reported that suspected overdoses jumped nationally by 18% in March, 29% in April, and 42% in May. This fits a nationwide pattern of excess deaths--deaths above the typical number anticipated by the CDC--unrelated to coronavirus, such as the increased toll from heart attacks, strokes, and cancer, all as our medical infrastructure is pushed to its limits.
There has never been a more critical time to provide medication for addiction treatment (MAT) for people with opioid use disorder (OUD).
There has never been a more critical time to provide medication for addiction treatment (MAT) for people with opioid use disorder (OUD). MAT consists of three FDA-approved medications--methadone, buprenorphine, and naltrexone--that treat OUD, the disease at the root of opioid addiction. MAT is basic healthcare and a cornerstone of care for tens of thousands of people in our communities who have OUD.
The need for MAT is particularly strong in jails and prisons: Without access to their medication, recently incarcerated people are left with few tools to battle their addiction. If provided with MAT, they are 74% less likely than people who are deprived of MAT to die of any cause while they are still incarcerated, and 85% less likely than people who are deprived of MAT to die of an overdose in the weeks after their release. Yet in the face of these stark numbers, 98% of jails and prisons still deny this lifesaving treatment to incarcerated people.
The small but growing number of prisons and jails that have implemented programs to provide MAT to incarcerated people with OUD have seen success. One study of the Rhode Island prison system, which was among the first to implement a robust MAT program, found that providing MAT reduced post-release deaths by 60%, and all opioid related deaths in the entire state by 12%. Sheriff Chris Donelan in Franklin County, Massachusetts reported a reduction in recidivism, overdose deaths, disciplinary concerns, and contraband after providing access to MAT.
In addition to saving lives, courts have found that providing MAT is a constitutional and civil right for incarcerated people. The Eighth Amendment to the U.S. Constitution bans "cruel and unusual punishment," which the Supreme Court has interpreted as prohibiting "deliberate indifference to serious medical needs." Further, the Americans with Disabilities Act (ADA) prohibits discrimination in public services, such as healthcare in jails, based upon a recognized disability, like OUD.
Last year, the First Circuit affirmed a ruling in the District of Maine under the ADA that a jail could not deny a woman serving a 40-day sentence access to the MAT prescribed to her by a doctor. This followed a decision by the District of Massachusetts that required a jail to provide an incarcerated individual with his prescribed MAT dose throughout his time in custody, holding that the denial of his medically necessary MAT was likely cruel and unusual punishment in violation of the Eighth Amendment as well as unlawful disability discrimination under the ADA.
As of July 22, more than 100,000 incarcerated people have been infected with Covid-19 and more than 760 have died. Even in the best of times, incarcerated people often receive substandard medical care, or no care at all. As Covid-19 cases make a resurgence in parts of the U.S. and continue to dramatically spike in jails, prisons, and detention facilities across the country, it has never been more important to provide evidence-based care for people with opioid use disorder in order to conserve hospital resources and save lives.
Our prisons and jails aren't designed to be drug rehab centers, and we must stop using them as such.
Our prisons and jails aren't designed to be drug rehab centers, and we must stop using them as such. Keeping people out of jail in the first place by making sure that they have reliable access to MAT both inside jails and prisons, and when they are out in the community, will help stop the rampant spread of Covid-19 and reduce the burden on our medical system.
Further, as researchers have pointed out, the symptoms of opioid withdrawal and Covid-19 can overlap. Without access to MAT for OUD, there is an increased danger that prison officials will miss suspected cases of Covid-19, assuming that the symptoms exhibited are a result of opioid withdrawal, when in fact they are symptoms of Covid-19. This creates a danger that a positive Covid-19 case could be missed by a correctional facility, allowing a positive individual to spread the disease to others with whom they share close quarters. The answer to this problem should never be solitary confinement.
Denying incarcerated people access to MAT adds a strain on the American healthcare system, even in the best of times. Nearly one quarter of America's prison and jail population of 2.2 million have OUD. During this crisis, it is even more imperative that people with OUD get access to the MAT they need. Instead of letting unlawful and scientifically unsound jail policies fill our hospital beds with people experiencing post-release overdoses, let's provide MAT to incarcerated people and use our hospitals to fight the Covid-19 crisis at hand.
We've already seen the federal government take some positive steps once thought impossible. This includes letting MAT patients take home their buprenorphine for 28 days in order to limit social contact while maintaining MAT treatment. While the federal Bureau of Prisons (BOP) has taken steps to expand access to MAT, the Department of Justice has supported recommendations from the Government Accountability Office aimed at making BOP improve the implementation of its MAT program so that it can serve everyone in need. It is time for Congress and state legislatures around the country to follow the lead of states like Rhode Island, and require MAT in all jails and prisons for everyone it is clinically appropriate for.

