

SUBSCRIBE TO OUR FREE NEWSLETTER
Daily news & progressive opinion—funded by the people, not the corporations—delivered straight to your inbox.
5
#000000
#FFFFFF
To donate by check, phone, or other method, see our More Ways to Give page.
Daily news & progressive opinion—funded by the people, not the corporations—delivered straight to your inbox.
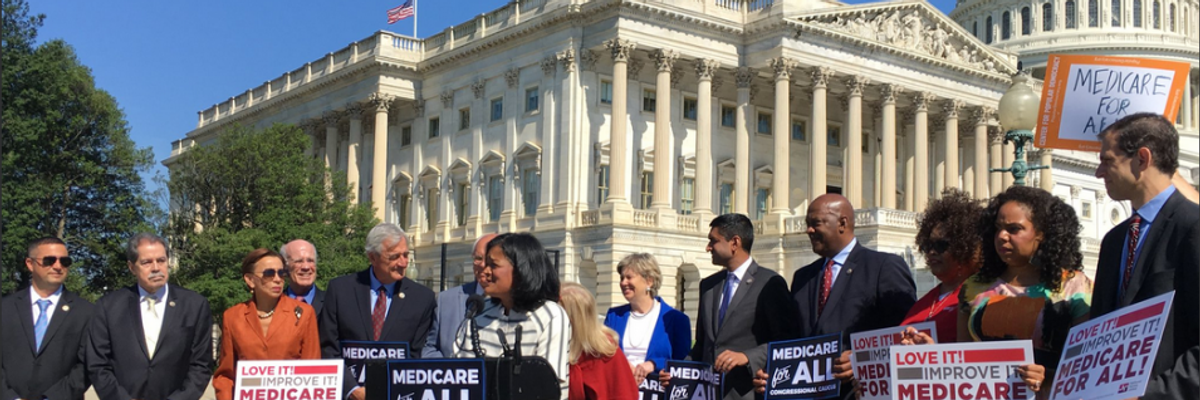
Rep. Pramila Jayapal introducing the new Medicare for All Caucus during a Capitol Hill press conference in July of 2018. (Photo: Rep. Pramila Jayapal/Twitter)
Dear Congresswoman Jayapal,
Thank you for your hard work and leadership as the new lead sponsor of the forthcoming Medicare for All Act of 2019. As health care providers and health justice advocates, we look forward to working with you to grow support for the bill and ensure its future passage.
"There is no place for profit in a humane and efficient national health program."
We applaud your efforts to improve the legislation from previous versions by including guaranteed access to vital services such as reproductive health and long-term care. However, we have identified two key policy provisions that must be addressed in the final bill: 1) the explicit prohibition and buyout of investor-owned, for-profit health facilities, and 2) the explicit inclusion of coverage for every resident of the U.S., regardless of immigration or citizenship status.
1. As part of a transition to a Medicare-for-all system, for-profit health facilities should be converted to nonprofit governance and their owners compensated for past investments.
There is no place for profit in a humane and efficient national health program. For-profit providers (including hospitals, dialysis centers, nursing homes, home care agencies, and hospices) have been shown to provide inferior care at inflated prices and are more likely to bend care to profitability. For-profit hospitals spend less on nurses and other clinical aspects of care, but more on administration and financial management, compared to nonprofits. For-profit nursing homes are cited for quality deficiencies 28 percent more often than nonprofits, and for deficiencies that place residents in immediate jeopardy 53 percent more frequently. Investor-owned home care agencies cost Medicare $752 more per patient than nonprofit agencies, while providing worse care. In addition, investor-owned chains have often been cited for questionable business practices and have been repeatedly implicated in large-scale fraud.
To achieve a fully nonprofit health system, Medicare for all legislation should include plans for the government to "buy out" investors in for-profit institutions. Researchers estimate the fair market value of investor-owned facilities covered by a buyout to be $150 billion at most. Using Treasury Bill financing over 15 years at the current interest rate of 3 percent would cost the government about $12.75 billion annually, equivalent to about 1 percent of annual hospital costs. Even in the short term, these costs would be offset by eliminating what we currently waste on investor profits. For example, total profits of just three investor-owned firms (HCA, DaVita and Fresenius) totaled more than $6 billion in 2017. For the sake of both patient health and cost savings, we cannot afford to let investor-owned facilities participate in a Medicare for all system.
2. A future Medicare for all program must include everyone living in the U.S., regardless of immigration or citizenship status.
Aside from humanitarian concerns, excluding anyone in the U.S. from a national health plan only adds waste and unnecessary administrative costs. Immigrants are often used as a scapegoat for skyrocketing health costs, but studies show that instead of draining our health care dollars, immigrants subsidize and maintain our health care system.
"Aside from humanitarian concerns, excluding anyone in the U.S. from a national health plan only adds waste and unnecessary administrative costs."
Between 2002 and 2009, immigrants contributed $115 billion more to the Medicare Trust Fund than they used in health care. Because of their lower utilization costs, immigrants also heavily subsidize private insurance for U.S.-born residents. A single-payer bill must explicitly include both documented and undocumented immigrants, and not leave eligibility up to administrative whims.
As medical students and physicians, we strongly believe that a single-payer program is the only solution to our country's failing health care system. However, to ensure the long-term success of Medicare for All, we must get the policy details right, including a ban on for-profit health facilities with a planned buyout of investors, and the inclusion of every U.S. resident, regardless of immigration status.
Sincerely,
Christopher Cai, Medical Student
Isabel Ostrer, Medical Student
Ana Malinow, MD
Dear Common Dreams reader, It’s been nearly 30 years since I co-founded Common Dreams with my late wife, Lina Newhouser. We had the radical notion that journalism should serve the public good, not corporate profits. It was clear to us from the outset what it would take to build such a project. No paid advertisements. No corporate sponsors. No millionaire publisher telling us what to think or do. Many people said we wouldn't last a year, but we proved those doubters wrong. Together with a tremendous team of journalists and dedicated staff, we built an independent media outlet free from the constraints of profits and corporate control. Our mission has always been simple: To inform. To inspire. To ignite change for the common good. Building Common Dreams was not easy. Our survival was never guaranteed. When you take on the most powerful forces—Wall Street greed, fossil fuel industry destruction, Big Tech lobbyists, and uber-rich oligarchs who have spent billions upon billions rigging the economy and democracy in their favor—the only bulwark you have is supporters who believe in your work. But here’s the urgent message from me today. It's never been this bad out there. And it's never been this hard to keep us going. At the very moment Common Dreams is most needed, the threats we face are intensifying. We need your support now more than ever. We don't accept corporate advertising and never will. We don't have a paywall because we don't think people should be blocked from critical news based on their ability to pay. Everything we do is funded by the donations of readers like you. When everyone does the little they can afford, we are strong. But if that support retreats or dries up, so do we. Will you donate now to make sure Common Dreams not only survives but thrives? —Craig Brown, Co-founder |
Dear Congresswoman Jayapal,
Thank you for your hard work and leadership as the new lead sponsor of the forthcoming Medicare for All Act of 2019. As health care providers and health justice advocates, we look forward to working with you to grow support for the bill and ensure its future passage.
"There is no place for profit in a humane and efficient national health program."
We applaud your efforts to improve the legislation from previous versions by including guaranteed access to vital services such as reproductive health and long-term care. However, we have identified two key policy provisions that must be addressed in the final bill: 1) the explicit prohibition and buyout of investor-owned, for-profit health facilities, and 2) the explicit inclusion of coverage for every resident of the U.S., regardless of immigration or citizenship status.
1. As part of a transition to a Medicare-for-all system, for-profit health facilities should be converted to nonprofit governance and their owners compensated for past investments.
There is no place for profit in a humane and efficient national health program. For-profit providers (including hospitals, dialysis centers, nursing homes, home care agencies, and hospices) have been shown to provide inferior care at inflated prices and are more likely to bend care to profitability. For-profit hospitals spend less on nurses and other clinical aspects of care, but more on administration and financial management, compared to nonprofits. For-profit nursing homes are cited for quality deficiencies 28 percent more often than nonprofits, and for deficiencies that place residents in immediate jeopardy 53 percent more frequently. Investor-owned home care agencies cost Medicare $752 more per patient than nonprofit agencies, while providing worse care. In addition, investor-owned chains have often been cited for questionable business practices and have been repeatedly implicated in large-scale fraud.
To achieve a fully nonprofit health system, Medicare for all legislation should include plans for the government to "buy out" investors in for-profit institutions. Researchers estimate the fair market value of investor-owned facilities covered by a buyout to be $150 billion at most. Using Treasury Bill financing over 15 years at the current interest rate of 3 percent would cost the government about $12.75 billion annually, equivalent to about 1 percent of annual hospital costs. Even in the short term, these costs would be offset by eliminating what we currently waste on investor profits. For example, total profits of just three investor-owned firms (HCA, DaVita and Fresenius) totaled more than $6 billion in 2017. For the sake of both patient health and cost savings, we cannot afford to let investor-owned facilities participate in a Medicare for all system.
2. A future Medicare for all program must include everyone living in the U.S., regardless of immigration or citizenship status.
Aside from humanitarian concerns, excluding anyone in the U.S. from a national health plan only adds waste and unnecessary administrative costs. Immigrants are often used as a scapegoat for skyrocketing health costs, but studies show that instead of draining our health care dollars, immigrants subsidize and maintain our health care system.
"Aside from humanitarian concerns, excluding anyone in the U.S. from a national health plan only adds waste and unnecessary administrative costs."
Between 2002 and 2009, immigrants contributed $115 billion more to the Medicare Trust Fund than they used in health care. Because of their lower utilization costs, immigrants also heavily subsidize private insurance for U.S.-born residents. A single-payer bill must explicitly include both documented and undocumented immigrants, and not leave eligibility up to administrative whims.
As medical students and physicians, we strongly believe that a single-payer program is the only solution to our country's failing health care system. However, to ensure the long-term success of Medicare for All, we must get the policy details right, including a ban on for-profit health facilities with a planned buyout of investors, and the inclusion of every U.S. resident, regardless of immigration status.
Sincerely,
Christopher Cai, Medical Student
Isabel Ostrer, Medical Student
Ana Malinow, MD
Dear Congresswoman Jayapal,
Thank you for your hard work and leadership as the new lead sponsor of the forthcoming Medicare for All Act of 2019. As health care providers and health justice advocates, we look forward to working with you to grow support for the bill and ensure its future passage.
"There is no place for profit in a humane and efficient national health program."
We applaud your efforts to improve the legislation from previous versions by including guaranteed access to vital services such as reproductive health and long-term care. However, we have identified two key policy provisions that must be addressed in the final bill: 1) the explicit prohibition and buyout of investor-owned, for-profit health facilities, and 2) the explicit inclusion of coverage for every resident of the U.S., regardless of immigration or citizenship status.
1. As part of a transition to a Medicare-for-all system, for-profit health facilities should be converted to nonprofit governance and their owners compensated for past investments.
There is no place for profit in a humane and efficient national health program. For-profit providers (including hospitals, dialysis centers, nursing homes, home care agencies, and hospices) have been shown to provide inferior care at inflated prices and are more likely to bend care to profitability. For-profit hospitals spend less on nurses and other clinical aspects of care, but more on administration and financial management, compared to nonprofits. For-profit nursing homes are cited for quality deficiencies 28 percent more often than nonprofits, and for deficiencies that place residents in immediate jeopardy 53 percent more frequently. Investor-owned home care agencies cost Medicare $752 more per patient than nonprofit agencies, while providing worse care. In addition, investor-owned chains have often been cited for questionable business practices and have been repeatedly implicated in large-scale fraud.
To achieve a fully nonprofit health system, Medicare for all legislation should include plans for the government to "buy out" investors in for-profit institutions. Researchers estimate the fair market value of investor-owned facilities covered by a buyout to be $150 billion at most. Using Treasury Bill financing over 15 years at the current interest rate of 3 percent would cost the government about $12.75 billion annually, equivalent to about 1 percent of annual hospital costs. Even in the short term, these costs would be offset by eliminating what we currently waste on investor profits. For example, total profits of just three investor-owned firms (HCA, DaVita and Fresenius) totaled more than $6 billion in 2017. For the sake of both patient health and cost savings, we cannot afford to let investor-owned facilities participate in a Medicare for all system.
2. A future Medicare for all program must include everyone living in the U.S., regardless of immigration or citizenship status.
Aside from humanitarian concerns, excluding anyone in the U.S. from a national health plan only adds waste and unnecessary administrative costs. Immigrants are often used as a scapegoat for skyrocketing health costs, but studies show that instead of draining our health care dollars, immigrants subsidize and maintain our health care system.
"Aside from humanitarian concerns, excluding anyone in the U.S. from a national health plan only adds waste and unnecessary administrative costs."
Between 2002 and 2009, immigrants contributed $115 billion more to the Medicare Trust Fund than they used in health care. Because of their lower utilization costs, immigrants also heavily subsidize private insurance for U.S.-born residents. A single-payer bill must explicitly include both documented and undocumented immigrants, and not leave eligibility up to administrative whims.
As medical students and physicians, we strongly believe that a single-payer program is the only solution to our country's failing health care system. However, to ensure the long-term success of Medicare for All, we must get the policy details right, including a ban on for-profit health facilities with a planned buyout of investors, and the inclusion of every U.S. resident, regardless of immigration status.
Sincerely,
Christopher Cai, Medical Student
Isabel Ostrer, Medical Student
Ana Malinow, MD

