

SUBSCRIBE TO OUR FREE NEWSLETTER
Daily news & progressive opinion—funded by the people, not the corporations—delivered straight to your inbox.
5
#000000
#FFFFFF
To donate by check, phone, or other method, see our More Ways to Give page.
Daily news & progressive opinion—funded by the people, not the corporations—delivered straight to your inbox.
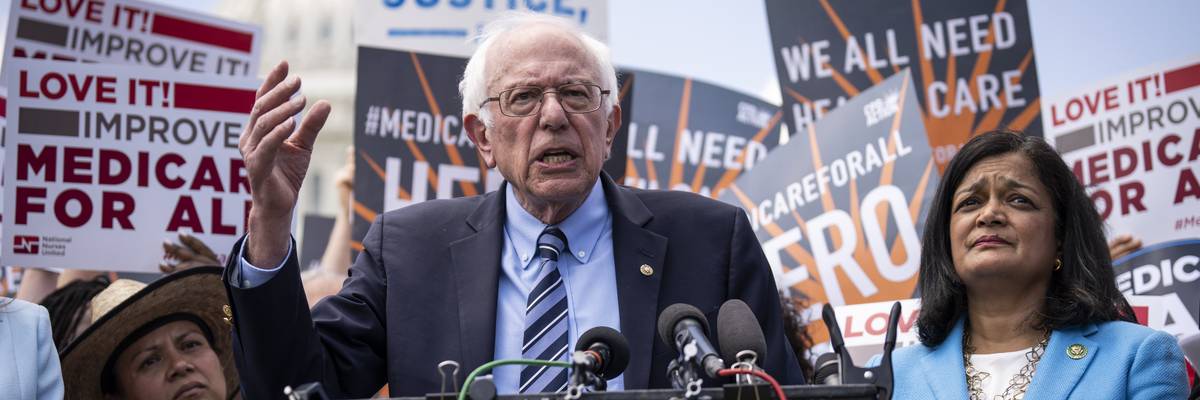
Sen. Bernie Sanders (I-Vt.) speaks alongside Rep. Pramila Jayapal (D-Wash.) during a news conference to announce the re-introduction of the Medicare For All Act of 2023, outside the U.S. Capitol on May 17, 2023 in Washington, D.C.
The only two peer-reviewed medical articles on the issue in the last 30 years came to the same conclusion: Medicare for All will save money, by removing unnecessary paperwork and insurance company profits, lowering drug costs, and other factors.
On Wednesday, Medicare for All legislation was introduced in the U.S. Senate and House, by Senator Bernie Sanders (I-Vt.) and Congresswoman Pramila Jayapal (D-Wash.). The bills use public financing to provide excellent insurance (including dental, vision, and long-term care) for everyone, with minimal cost-sharing.
A central question is affordability. Will Medicare for All raise or lower healthcare costs in the United States? Is it affordable?
We led two academic teams that published scientific papers to address this, the only peer-reviewed medical articles on this topic in the last 30 years. We worked separately, at Yale University and the University of California.
We think it’s time to retire doubts about the net cost of single payer or Medicare for All. The evidence for big savings is real.
We came to the same conclusion: Yes, Medicare for All will save money, by removing unnecessary paperwork and insurance company profits, lowering drug costs, and other factors. These savings will more than offset the cost of improving coverage and expanding it to everyone.
In the University of California review we found that 19 of 22 past analyses of single-payer or Medicare-for-All plans, from 1990 to 2018, projected net savings in year one. The median expected savings was 3.5%. That equals $120 billion in net savings for the U.S., with increases over time due to controls on spending growth. The exact savings varied across studies due to differences in anticipated reductions in paperwork and drug costs.
In the Yale study, using the latest available data to create a new analysis, we estimated that the Sanders bill would save more than $450 billion per year (13% of all health spending) while preventing tens of thousands of deaths compared with the status quo. In addition, the quality and productivity of our lives will be improved by Medicare for All.
What does it mean that these two studies came to the same basic conclusion?
The Congressional Budget Office also estimated net savings from single payer.
What's the difference between these studies, which conclude that single payer would save money, and other studies that conclude it would not?
By the way, these net savings are underestimated. None of these studies, not even the most recent one, had access to new evidence suggesting that universal coverage expansions have historically led to modest or even zero increases in healthcare use. The newly covered individuals use more health care, to be sure, but at the same time, doctors provide a bit less unnecessary care to the well-off and well-insured. This means that overall increases are minimal, and universal coverage adds less cost.
How should this evidence change the discussion?
We think it’s time to retire doubts about the net cost of single-payer or Medicare for All. The evidence for big savings is real.
Here’s the headline: Medicare for All saves both money and lives. It’s a no-brainer.
Dear Common Dreams reader, It’s been nearly 30 years since I co-founded Common Dreams with my late wife, Lina Newhouser. We had the radical notion that journalism should serve the public good, not corporate profits. It was clear to us from the outset what it would take to build such a project. No paid advertisements. No corporate sponsors. No millionaire publisher telling us what to think or do. Many people said we wouldn't last a year, but we proved those doubters wrong. Together with a tremendous team of journalists and dedicated staff, we built an independent media outlet free from the constraints of profits and corporate control. Our mission has always been simple: To inform. To inspire. To ignite change for the common good. Building Common Dreams was not easy. Our survival was never guaranteed. When you take on the most powerful forces—Wall Street greed, fossil fuel industry destruction, Big Tech lobbyists, and uber-rich oligarchs who have spent billions upon billions rigging the economy and democracy in their favor—the only bulwark you have is supporters who believe in your work. But here’s the urgent message from me today. It's never been this bad out there. And it's never been this hard to keep us going. At the very moment Common Dreams is most needed, the threats we face are intensifying. We need your support now more than ever. We don't accept corporate advertising and never will. We don't have a paywall because we don't think people should be blocked from critical news based on their ability to pay. Everything we do is funded by the donations of readers like you. When everyone does the little they can afford, we are strong. But if that support retreats or dries up, so do we. Will you donate now to make sure Common Dreams not only survives but thrives? —Craig Brown, Co-founder |
On Wednesday, Medicare for All legislation was introduced in the U.S. Senate and House, by Senator Bernie Sanders (I-Vt.) and Congresswoman Pramila Jayapal (D-Wash.). The bills use public financing to provide excellent insurance (including dental, vision, and long-term care) for everyone, with minimal cost-sharing.
A central question is affordability. Will Medicare for All raise or lower healthcare costs in the United States? Is it affordable?
We led two academic teams that published scientific papers to address this, the only peer-reviewed medical articles on this topic in the last 30 years. We worked separately, at Yale University and the University of California.
We think it’s time to retire doubts about the net cost of single payer or Medicare for All. The evidence for big savings is real.
We came to the same conclusion: Yes, Medicare for All will save money, by removing unnecessary paperwork and insurance company profits, lowering drug costs, and other factors. These savings will more than offset the cost of improving coverage and expanding it to everyone.
In the University of California review we found that 19 of 22 past analyses of single-payer or Medicare-for-All plans, from 1990 to 2018, projected net savings in year one. The median expected savings was 3.5%. That equals $120 billion in net savings for the U.S., with increases over time due to controls on spending growth. The exact savings varied across studies due to differences in anticipated reductions in paperwork and drug costs.
In the Yale study, using the latest available data to create a new analysis, we estimated that the Sanders bill would save more than $450 billion per year (13% of all health spending) while preventing tens of thousands of deaths compared with the status quo. In addition, the quality and productivity of our lives will be improved by Medicare for All.
What does it mean that these two studies came to the same basic conclusion?
The Congressional Budget Office also estimated net savings from single payer.
What's the difference between these studies, which conclude that single payer would save money, and other studies that conclude it would not?
By the way, these net savings are underestimated. None of these studies, not even the most recent one, had access to new evidence suggesting that universal coverage expansions have historically led to modest or even zero increases in healthcare use. The newly covered individuals use more health care, to be sure, but at the same time, doctors provide a bit less unnecessary care to the well-off and well-insured. This means that overall increases are minimal, and universal coverage adds less cost.
How should this evidence change the discussion?
We think it’s time to retire doubts about the net cost of single-payer or Medicare for All. The evidence for big savings is real.
Here’s the headline: Medicare for All saves both money and lives. It’s a no-brainer.
On Wednesday, Medicare for All legislation was introduced in the U.S. Senate and House, by Senator Bernie Sanders (I-Vt.) and Congresswoman Pramila Jayapal (D-Wash.). The bills use public financing to provide excellent insurance (including dental, vision, and long-term care) for everyone, with minimal cost-sharing.
A central question is affordability. Will Medicare for All raise or lower healthcare costs in the United States? Is it affordable?
We led two academic teams that published scientific papers to address this, the only peer-reviewed medical articles on this topic in the last 30 years. We worked separately, at Yale University and the University of California.
We think it’s time to retire doubts about the net cost of single payer or Medicare for All. The evidence for big savings is real.
We came to the same conclusion: Yes, Medicare for All will save money, by removing unnecessary paperwork and insurance company profits, lowering drug costs, and other factors. These savings will more than offset the cost of improving coverage and expanding it to everyone.
In the University of California review we found that 19 of 22 past analyses of single-payer or Medicare-for-All plans, from 1990 to 2018, projected net savings in year one. The median expected savings was 3.5%. That equals $120 billion in net savings for the U.S., with increases over time due to controls on spending growth. The exact savings varied across studies due to differences in anticipated reductions in paperwork and drug costs.
In the Yale study, using the latest available data to create a new analysis, we estimated that the Sanders bill would save more than $450 billion per year (13% of all health spending) while preventing tens of thousands of deaths compared with the status quo. In addition, the quality and productivity of our lives will be improved by Medicare for All.
What does it mean that these two studies came to the same basic conclusion?
The Congressional Budget Office also estimated net savings from single payer.
What's the difference between these studies, which conclude that single payer would save money, and other studies that conclude it would not?
By the way, these net savings are underestimated. None of these studies, not even the most recent one, had access to new evidence suggesting that universal coverage expansions have historically led to modest or even zero increases in healthcare use. The newly covered individuals use more health care, to be sure, but at the same time, doctors provide a bit less unnecessary care to the well-off and well-insured. This means that overall increases are minimal, and universal coverage adds less cost.
How should this evidence change the discussion?
We think it’s time to retire doubts about the net cost of single-payer or Medicare for All. The evidence for big savings is real.
Here’s the headline: Medicare for All saves both money and lives. It’s a no-brainer.

