SUBSCRIBE TO OUR FREE NEWSLETTER
Daily news & progressive opinion—funded by the people, not the corporations—delivered straight to your inbox.
5
#000000
#FFFFFF
To donate by check, phone, or other method, see our More Ways to Give page.
Daily news & progressive opinion—funded by the people, not the corporations—delivered straight to your inbox.
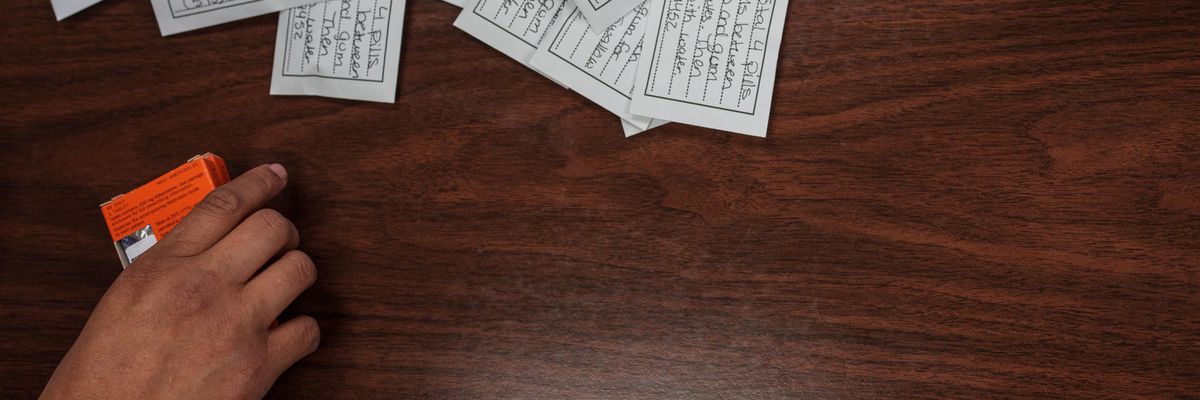
Doses of Mifepristone, the abortion pill, and Misoprostol, which is taken the day after to cause cramping and bleeding to empty the uterus, are pictured at Dr. Franz Theards Womens Reproductive Clinic in Santa Teresa, New Mexico, on May 7, 2022.
We need more people who believe in abortion as a human right to stand up for telemedicine abortion and protect access to mifepristone.
To paraphrase Charles Dickens, 2023 has been the “best of times and the worst of times” for abortion rights in America. Where you live, how much money you have, and whether you’re more than six weeks pregnant determine whether you can access your human rights.
The best news this year is that telemedicine abortion shield laws came to full fruition in five states. These new laws provide medical providers with protection from criminal and civil charges or license revocation so they can provide abortion pills by telemedicine nationwide.
As a result, telemedicine from a licensed clinician is now available in all 50 states. After speaking to providers across the country, I learned that more than 6,000 women per month are using this method in the states where it’s the worst of times for abortion rights.
What’s at stake in the 2024 presidential election is the tiny abortion pill that makes a big difference.
Telemedicine abortion from shield states is a bright light that contrasts with the grim reality of abortion access.
Since Roe v. Wade was toppled in 2022, the majority of American women of reproductive age live in states that are hostile toward abortion rights. Fourteen states have banned abortion in almost all circumstances. Other states such as Georgia and South Carolina give the illusion of allowing early abortion before six weeks when in practice many women do not even know yet that they are pregnant.
When abortion is criminalized, even lifesaving exceptions are generally useless. In Texas, 22 women have come forward to sue after they were denied care when their lives were at risk. In a second Texas lawsuit, the state Supreme Court allowed a hospital to deny a woman an abortion after severe fetal anomalies threatened her health and future fertility.
We have seen that when abortion is banned, women in Ireland, Poland, El Salvador, Kenya, and elsewhere did not survive. Already the U.S. has one of the highest maternal mortality rates among wealthy nations in the world, particularly for women of color. The bans simply exacerbate this risk.
The good news is that the majority of people know this is just plain wrong.
More than 60% of Americans supported legal abortion before Roe was overturned, and that number has only grown since the Dobbs v. Jackson verdict that overturned it. Americans have consistently voted in favor of abortion rights such as on ballot initiatives in Ohio, Kansas, and Michigan. Voters also have turned out in droves to support Democratic candidates who prioritize abortion rights such as in Virginia’s general legislative election and Wisconsin’s Supreme Court race this year.
But what’s at stake in the 2024 presidential election is the tiny abortion pill that makes a big difference. Next year the Supreme Court is expected to rule to significantly restrict access to mifepristone, a key abortion medication. So, whoever the next president puts in charge of the Food and Drug Administration will either sink or save us.
Mifepristone is the first pill in medication abortion, a proven safe and effective way to terminate a pregnancy through the first 11 weeks or possibly even later. The pill has been used globally for decades.
It is as safe as surgical abortion, less expensive, and allows a woman to have her abortion at home. That’s why more than 50% of American women having legal abortions chose it before Dobbs—and anecdotal evidence is that many more are doing so now—and more than three-quarters do so in Europe. Mifepristone provides essential abortion access.
Yet, before this year, only women who lived in, or could travel to, abortion-friendly states were able to get pills; geography was destiny. Now five abortion-friendly states—Colorado, Massachusetts, New York, Vermont, Washington, and soon California—have telemedicine abortion shield laws that are leveling the playing field nationwide.
As a result, for only $150 women can receive certified medications from a licensed provider without having to travel hundreds of miles, make child care arrangements, miss work or school, or make excuses for leaving the state. Telemedicine’s safety, convenience and lower cost make it an extremely popular alternative—even in states where abortion clinics still exist.
I’ve long known telemedicine abortion is essential because I’ve seen women in Ireland, where abortion was once illegal, forced to travel abroad to access safe services on what was euphemistically called the “ Irish Journey.” That same kind of difficult, expensive, and isolating journey is now happening for women in America.
A woman from Mississippi whose advocate I spoke with fled domestic violence and was living in a motel with her toddler and a baby when she realized she was pregnant. By using telemedicine, she avoided leaving her children behind for a six-hour drive to pick up her abortion pills in a neighboring state. Telemedicine abortion offers an option for those who desperately need it, as well as for those who simply choose it.
But doctors in states with shield laws still need help operating under current conditions and amid the continued threats to their practices and mifepristone’s availability. They need affordable, comprehensive, medical malpractice insurance; legal defense support to navigate the novelty of these shield laws; and political support from additional states passing shield laws. Most of all, they need help covering the cost of the pills for the many patients who can’t afford $150 and are not eligible for Medicaid or traditional abortion fund support.
Telemedicine abortion is at the forefront of what modern abortion access could look like, and it’s an exciting moment. We need more people who believe in abortion as a human right to stand up for telemedicine abortion. And we must all vote and work to protect access to mifepristone regardless of how the Supreme Court rules next year.
Dear Common Dreams reader, It’s been nearly 30 years since I co-founded Common Dreams with my late wife, Lina Newhouser. We had the radical notion that journalism should serve the public good, not corporate profits. It was clear to us from the outset what it would take to build such a project. No paid advertisements. No corporate sponsors. No millionaire publisher telling us what to think or do. Many people said we wouldn't last a year, but we proved those doubters wrong. Together with a tremendous team of journalists and dedicated staff, we built an independent media outlet free from the constraints of profits and corporate control. Our mission has always been simple: To inform. To inspire. To ignite change for the common good. Building Common Dreams was not easy. Our survival was never guaranteed. When you take on the most powerful forces—Wall Street greed, fossil fuel industry destruction, Big Tech lobbyists, and uber-rich oligarchs who have spent billions upon billions rigging the economy and democracy in their favor—the only bulwark you have is supporters who believe in your work. But here’s the urgent message from me today. It's never been this bad out there. And it's never been this hard to keep us going. At the very moment Common Dreams is most needed, the threats we face are intensifying. We need your support now more than ever. We don't accept corporate advertising and never will. We don't have a paywall because we don't think people should be blocked from critical news based on their ability to pay. Everything we do is funded by the donations of readers like you. When everyone does the little they can afford, we are strong. But if that support retreats or dries up, so do we. Will you donate now to make sure Common Dreams not only survives but thrives? —Craig Brown, Co-founder |
To paraphrase Charles Dickens, 2023 has been the “best of times and the worst of times” for abortion rights in America. Where you live, how much money you have, and whether you’re more than six weeks pregnant determine whether you can access your human rights.
The best news this year is that telemedicine abortion shield laws came to full fruition in five states. These new laws provide medical providers with protection from criminal and civil charges or license revocation so they can provide abortion pills by telemedicine nationwide.
As a result, telemedicine from a licensed clinician is now available in all 50 states. After speaking to providers across the country, I learned that more than 6,000 women per month are using this method in the states where it’s the worst of times for abortion rights.
What’s at stake in the 2024 presidential election is the tiny abortion pill that makes a big difference.
Telemedicine abortion from shield states is a bright light that contrasts with the grim reality of abortion access.
Since Roe v. Wade was toppled in 2022, the majority of American women of reproductive age live in states that are hostile toward abortion rights. Fourteen states have banned abortion in almost all circumstances. Other states such as Georgia and South Carolina give the illusion of allowing early abortion before six weeks when in practice many women do not even know yet that they are pregnant.
When abortion is criminalized, even lifesaving exceptions are generally useless. In Texas, 22 women have come forward to sue after they were denied care when their lives were at risk. In a second Texas lawsuit, the state Supreme Court allowed a hospital to deny a woman an abortion after severe fetal anomalies threatened her health and future fertility.
We have seen that when abortion is banned, women in Ireland, Poland, El Salvador, Kenya, and elsewhere did not survive. Already the U.S. has one of the highest maternal mortality rates among wealthy nations in the world, particularly for women of color. The bans simply exacerbate this risk.
The good news is that the majority of people know this is just plain wrong.
More than 60% of Americans supported legal abortion before Roe was overturned, and that number has only grown since the Dobbs v. Jackson verdict that overturned it. Americans have consistently voted in favor of abortion rights such as on ballot initiatives in Ohio, Kansas, and Michigan. Voters also have turned out in droves to support Democratic candidates who prioritize abortion rights such as in Virginia’s general legislative election and Wisconsin’s Supreme Court race this year.
But what’s at stake in the 2024 presidential election is the tiny abortion pill that makes a big difference. Next year the Supreme Court is expected to rule to significantly restrict access to mifepristone, a key abortion medication. So, whoever the next president puts in charge of the Food and Drug Administration will either sink or save us.
Mifepristone is the first pill in medication abortion, a proven safe and effective way to terminate a pregnancy through the first 11 weeks or possibly even later. The pill has been used globally for decades.
It is as safe as surgical abortion, less expensive, and allows a woman to have her abortion at home. That’s why more than 50% of American women having legal abortions chose it before Dobbs—and anecdotal evidence is that many more are doing so now—and more than three-quarters do so in Europe. Mifepristone provides essential abortion access.
Yet, before this year, only women who lived in, or could travel to, abortion-friendly states were able to get pills; geography was destiny. Now five abortion-friendly states—Colorado, Massachusetts, New York, Vermont, Washington, and soon California—have telemedicine abortion shield laws that are leveling the playing field nationwide.
As a result, for only $150 women can receive certified medications from a licensed provider without having to travel hundreds of miles, make child care arrangements, miss work or school, or make excuses for leaving the state. Telemedicine’s safety, convenience and lower cost make it an extremely popular alternative—even in states where abortion clinics still exist.
I’ve long known telemedicine abortion is essential because I’ve seen women in Ireland, where abortion was once illegal, forced to travel abroad to access safe services on what was euphemistically called the “ Irish Journey.” That same kind of difficult, expensive, and isolating journey is now happening for women in America.
A woman from Mississippi whose advocate I spoke with fled domestic violence and was living in a motel with her toddler and a baby when she realized she was pregnant. By using telemedicine, she avoided leaving her children behind for a six-hour drive to pick up her abortion pills in a neighboring state. Telemedicine abortion offers an option for those who desperately need it, as well as for those who simply choose it.
But doctors in states with shield laws still need help operating under current conditions and amid the continued threats to their practices and mifepristone’s availability. They need affordable, comprehensive, medical malpractice insurance; legal defense support to navigate the novelty of these shield laws; and political support from additional states passing shield laws. Most of all, they need help covering the cost of the pills for the many patients who can’t afford $150 and are not eligible for Medicaid or traditional abortion fund support.
Telemedicine abortion is at the forefront of what modern abortion access could look like, and it’s an exciting moment. We need more people who believe in abortion as a human right to stand up for telemedicine abortion. And we must all vote and work to protect access to mifepristone regardless of how the Supreme Court rules next year.
To paraphrase Charles Dickens, 2023 has been the “best of times and the worst of times” for abortion rights in America. Where you live, how much money you have, and whether you’re more than six weeks pregnant determine whether you can access your human rights.
The best news this year is that telemedicine abortion shield laws came to full fruition in five states. These new laws provide medical providers with protection from criminal and civil charges or license revocation so they can provide abortion pills by telemedicine nationwide.
As a result, telemedicine from a licensed clinician is now available in all 50 states. After speaking to providers across the country, I learned that more than 6,000 women per month are using this method in the states where it’s the worst of times for abortion rights.
What’s at stake in the 2024 presidential election is the tiny abortion pill that makes a big difference.
Telemedicine abortion from shield states is a bright light that contrasts with the grim reality of abortion access.
Since Roe v. Wade was toppled in 2022, the majority of American women of reproductive age live in states that are hostile toward abortion rights. Fourteen states have banned abortion in almost all circumstances. Other states such as Georgia and South Carolina give the illusion of allowing early abortion before six weeks when in practice many women do not even know yet that they are pregnant.
When abortion is criminalized, even lifesaving exceptions are generally useless. In Texas, 22 women have come forward to sue after they were denied care when their lives were at risk. In a second Texas lawsuit, the state Supreme Court allowed a hospital to deny a woman an abortion after severe fetal anomalies threatened her health and future fertility.
We have seen that when abortion is banned, women in Ireland, Poland, El Salvador, Kenya, and elsewhere did not survive. Already the U.S. has one of the highest maternal mortality rates among wealthy nations in the world, particularly for women of color. The bans simply exacerbate this risk.
The good news is that the majority of people know this is just plain wrong.
More than 60% of Americans supported legal abortion before Roe was overturned, and that number has only grown since the Dobbs v. Jackson verdict that overturned it. Americans have consistently voted in favor of abortion rights such as on ballot initiatives in Ohio, Kansas, and Michigan. Voters also have turned out in droves to support Democratic candidates who prioritize abortion rights such as in Virginia’s general legislative election and Wisconsin’s Supreme Court race this year.
But what’s at stake in the 2024 presidential election is the tiny abortion pill that makes a big difference. Next year the Supreme Court is expected to rule to significantly restrict access to mifepristone, a key abortion medication. So, whoever the next president puts in charge of the Food and Drug Administration will either sink or save us.
Mifepristone is the first pill in medication abortion, a proven safe and effective way to terminate a pregnancy through the first 11 weeks or possibly even later. The pill has been used globally for decades.
It is as safe as surgical abortion, less expensive, and allows a woman to have her abortion at home. That’s why more than 50% of American women having legal abortions chose it before Dobbs—and anecdotal evidence is that many more are doing so now—and more than three-quarters do so in Europe. Mifepristone provides essential abortion access.
Yet, before this year, only women who lived in, or could travel to, abortion-friendly states were able to get pills; geography was destiny. Now five abortion-friendly states—Colorado, Massachusetts, New York, Vermont, Washington, and soon California—have telemedicine abortion shield laws that are leveling the playing field nationwide.
As a result, for only $150 women can receive certified medications from a licensed provider without having to travel hundreds of miles, make child care arrangements, miss work or school, or make excuses for leaving the state. Telemedicine’s safety, convenience and lower cost make it an extremely popular alternative—even in states where abortion clinics still exist.
I’ve long known telemedicine abortion is essential because I’ve seen women in Ireland, where abortion was once illegal, forced to travel abroad to access safe services on what was euphemistically called the “ Irish Journey.” That same kind of difficult, expensive, and isolating journey is now happening for women in America.
A woman from Mississippi whose advocate I spoke with fled domestic violence and was living in a motel with her toddler and a baby when she realized she was pregnant. By using telemedicine, she avoided leaving her children behind for a six-hour drive to pick up her abortion pills in a neighboring state. Telemedicine abortion offers an option for those who desperately need it, as well as for those who simply choose it.
But doctors in states with shield laws still need help operating under current conditions and amid the continued threats to their practices and mifepristone’s availability. They need affordable, comprehensive, medical malpractice insurance; legal defense support to navigate the novelty of these shield laws; and political support from additional states passing shield laws. Most of all, they need help covering the cost of the pills for the many patients who can’t afford $150 and are not eligible for Medicaid or traditional abortion fund support.
Telemedicine abortion is at the forefront of what modern abortion access could look like, and it’s an exciting moment. We need more people who believe in abortion as a human right to stand up for telemedicine abortion. And we must all vote and work to protect access to mifepristone regardless of how the Supreme Court rules next year.