

SUBSCRIBE TO OUR FREE NEWSLETTER
Daily news & progressive opinion—funded by the people, not the corporations—delivered straight to your inbox.
5
#000000
#FFFFFF
To donate by check, phone, or other method, see our More Ways to Give page.
Daily news & progressive opinion—funded by the people, not the corporations—delivered straight to your inbox.

The U.S. "has always accepted that we are the country that overpays relative to the rest of the world," said one health policy expert.
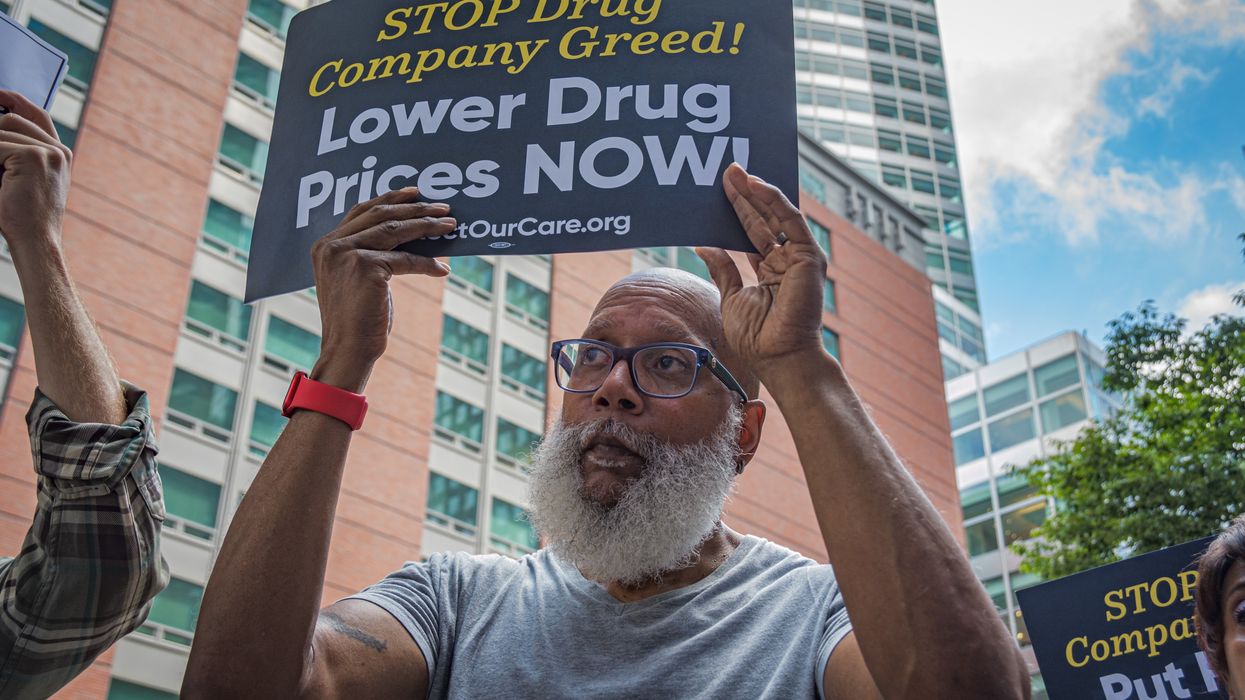
The Biden administration's Medicare drug price negotiations yielded lowered costs for 10 commonly used drugs, and the White House said last month that Americans would save an estimated $1.5 billion in out-of-pocket expenses thanks to the talks—but an analysis out Tuesday found that the U.S. will still be paying far more than other wealthy countries.
Reuters reviewed the maximum prices that Australia, Japan, Canada, and Sweden have agreed to pay for nine of the 10 drugs for which Medicare negotiated prices this year, and found that the U.S. will still be paying more than double the amount for the medications on average.
The new prices are set to go into effect on January 1, 2026, but two of the highest prices the U.S. will still pay are for Imbruvica, for blood cancers, and Stelara, for conditions including Crohn's disease and psoriasis.
Medicare will be charged $9,319 for a 30-day supply of the latter drug, compared to $4,607 in Sweden. For Stelara, the U.S. will pay $4,695 under the negotiated prices—more than four times the amount it costs in Sweden, Australia, and Canada.
For Enbrel, which treats conditions including arthritis, Medicare will pay $2,355 per month—far less than the list price of $7,106, but still more than $1,000 over what Sweden is charged: $709. Australia pays $573, while Canada pays $704, and Japan pays just over $300 for the drug.
"The government negotiations are especially significant for drugs where market forces were most limited and therefore had the least impact on producing price concessions."
Stacie Dusetzina, a professor of health policy at Vanderbilt University, told Reuters that the U.S. has "always accepted that we are the country that overpays relative to the rest of the world."
The analysis comes two weeks after the Brookings Institution published a review of the impact of the United States' first federal negotiations of prescription drug prices, finding that just three of the drugs which had little competition in the market accounted for more than half of the $6 billion the U.S. is expected to save in 2026.
"The government negotiations are especially significant for drugs where market forces were most limited and therefore had the least impact on producing price concessions," said Brookings.
Reuters noted that in other countries, prices generally come down over time, but U.S. drugmakers are able to raise prices annually and often extend patents by making small changes to medications, stopping less expensive generic versions from hitting the market and saving patients money.
Unlike in other wealthy countries, Johns Hopkins Bloomberg School of Public Health scientist Mariana Socal told Reuters, "the longer a drug is in the U.S. market, the more we pay."
With previous list prices well into the hundreds and thousands for the 10 drugs included in negotiations so far, Medicare agreed to pay close to $200 for a 30-day supply for drugs including Xarelto, Jardiance, and Farxiga—medications for which other governments examined by Reuters pay $78 or less, thanks to their longstanding negotiations.
The RAND Corporation found in a study in February that before the Medicare negotiations were included in the Inflation Reduction Act, U.S. health plans paid more than three times as much as other countries for brand-name drugs, even after discounts.
"A contributor to higher U.S. per capita drug spending is faster uptake of new and more expensive prescription drugs in the United States relative to other countries," wrote researchers at the London School of Economics in a study in 2013. "In contrast, the other OECD countries employed mechanisms such as health technology assessment and restrictions on patients' eligibility for new prescription drugs, and they required strict evidence of the value of new drugs."
The researchers suggested pharmaceutical companies in the U.S., like in other countries, should be required "to provide more evidence about the value of new drugs in relation to the cost" and negotiate prices accordingly.
As Merith Basey, executive director of Patients for Affordable Drugs, said in August after the results of the first round of negotiations were announced, advocates are still pushing for far more savings in upcoming talks between Medicare and drug manufacturers, which are expected to start next year.
"We remain committed to expanding the Medicare negotiation program to more drugs," said Basey last month, "and fighting for additional reforms to lower drug prices for all patients who need relief."

From the $35 insulin co-pay to capping insurance premium costs, the legislation has been health-changing and life-changing.
I was honored to be at the White House this month for the Inflation Reduction Act anniversary event, featuring Americans sharing their stories of saving money and saving lives.
Thank you to the millions of people fighting every day for lower drug prices, to Congress for passing the Inflation Reduction Act, U.S. Vice President Kamala Harris for casting the deciding vote in the Senate, and President Joe Biden for signing it into law.
Meet Bob Parant, from New York. He’s a 71-year-old man who has been living with type 1 diabetes for over fifty years. He lost his leg in 2010, and became eligible for Medicare. Before the Inflation Reduction Act, the last price Bob paid for a vial of insulin was $580, which was “horrendous.”
We have made so much progress on healthcare. But as everyone reading this knows, there is so much more to do.
Listen to Pam Parker, from Maryland: She’s a retired electrician, 62 years old, and has been diabetic since she was 30. “I had to decide, a lot of months, between mortgage, groceries, utilities, and other things… I would juggle my expenses, and really juggle my healthcare.. I would eat less, or ration my insulin to make it last.. I had high blood pressure, I fell into a coma, my kidneys failed… they told me I coded.”
Learn from Robin Craycroft, from Missouri: When she turned 65 and had access to Medicare, the pharmacist told her that one insulin for three months was $3,000. “Everything that we had planned, cancelled, and our life just changed. And I felt such guilt over that… We’re gonna spend $2,000 a month (two insulin vials) to keep me alive. You start going through, am I worth it? Should I do that to [my husband]?”
Hear Steven Hadfield, from North Carolina: “Before the $35 cap, sometimes you had to skip a dose, sometimes you had to not test yourself, watch what you eat because you couldn’t afford it…”
The $35 insulin co-pay cap for people on Medicare is just one of the health-changing and life-changing parts of the Inflation Reduction Act.
This year, people on Medicare have their out of pocket Part D drug costs capped at around $3,500. And next year, the maximum drops down to $2,000. This means seniors on a fixed income won’t have to choose medicine over food or housing or anything else. Also recommended adult vaccines such as the new shingles vaccine are now free for Medicare recipients.
Pharmaceutical companies that raise their prices higher than inflation are required to pay Medicare a rebate, to encourage them to stop price gouging patients. And in 2026, price negotiations for the first 10 drugs under Medicare go into effect: lowering the costs of those drugs for millions of Americans. The savings will continue for patients and taxpayers as more drug prices are negotiated each year.
But the Inflation Reduction Act doesn’t just help people on Medicare. Over 21 million Americans like me get their health insurance through the Affordable Care Act marketplaces. When I was diagnosed with stage 4 cancer in 2017, I did not qualify for financial help for insurance. Thankfully I was able to afford a plan anyway, and to pay the maximum deductible for that year. A bargain compared to the over half a million dollars it cost to save my life.
I am so grateful to still be here, and for the Affordable Care Act made truly more affordable to millions of working Americans like me.
The American Rescue Plan, and then the Inflation Reduction Act, provided financial help for health insurance to many more who needed it. This law caps the cost of premiums at no more than 8.5% of your income, meaning people—especially older folks who face higher premiums, or people in more expensive healthcare markets—don’t get penalized, and can still afford the care they need.
We have made so much progress on healthcare. But as everyone reading this knows, there is so much more to do.
First, we have to defend the advances in the Inflation Reduction Act. A new administration and a new Congress next year means everything we’ve gained could be on the chopping block.
Second, the health insurance tax credits piece expires in 2025. Without that renewal, millions of Americans would go back to being priced out of health insurance.
Third, the Medicare provisions such as the $35 insulin cap, the drug price negotiation, and more, need to be expanded to everyone.
We are grateful to still be here, and to keep fighting until every American can get the healthcare they need. We cannot go back.
The president’s Inflation Reduction Act contained several provisions affecting drug prices, including three that began to take effect in 2023.
Prices for prescription drugs in America average almost three times as much as in other major nations around the world. Even more, the companies that set those prices are doing everything they can to make sure they stay in the stratosphere: They’ve filed suit to overturn an upcoming reform, having Medicare negotiate the prices of some of the costliest and most commonly used drugs.
The makers don’t think they need to explain themselves, either. If they hadn’t been threatened with subpoenas, their CEOs would never have showed up to waffle their way through a Senate hearing on drug pricing earlier this year.
Lastly, the companies argue that critics of high prices should instead be praising the industry for all the research it carries out to make the drugs available in the first place—failing to mention, of course, the critical role that government funding regularly plays in the development of new drugs.
If you wonder how patients could be harmed by lower drug prices, feel free to ask the Pharmaceutical Research and Manufacturers of America.
A big contributor to insane drug prices is the billions spent on those incessant drug commercials. Hour after hour, eyes glazing over, TV watchers are bombarded with happy-time ads for Rinvoq, Skyrizi, Dupixent, Sanofi, Jardiance, on and on and then some.
Thank heaven for mute buttons; more to the point, thank heaven that the Biden administration is leading the way to somewhat less insanity.
The president’s Inflation Reduction Act contained several provisions affecting drug prices, including three that began to take effect in 2023. The bill capped the price of insulin at $35 a month, made some vaccines free, and required drug companies that raised prices faster than the rate of inflation to pay rebates to Medicare.
Here’s President Joe Biden taking a victory lap during his State of the Union address: “That’s not just saving seniors money, it’s saving taxpayers money. We cut the federal deficit by $160 billion because Medicare will no longer have to pay those exorbitant prices…”
Other cost-saving provisions are coming as well. Starting in 2025, out-of-pocket prescription drug costs for retirees covered under Medicare Part D will be capped at $2,000. Annual limits after 2025 will be adjusted based on inflation rates.
Medicare-negotiated drug prices, mentioned earlier, have an effective date of 2026 (unless, of course, they get derailed by Big Pharma). Negotiations between Medicare and the makers are already underway for the first 10 covered drugs; all by themselves, those 10 accounted for over $3.4 billion in out-of-pocket costs in 2022.
Drug prices could fall even more sharply under the terms of the proposed 2025 budget for the Department of Health and Human Services. Instead of Medicare-negotiated prices for 10 drugs, the number would rise to 50 per year.
Presidents also have the power to make things happen without congressional legislation, and a Biden executive order could result in allowing states to import lower-cost drugs in bulk from Canada. The Food and Drug Administration approved Florida’s request early this year, and other states are hoping to follow. (Full disclosure: Florida’s Republican Gov. Ron DeSantis and former President Donald Trump also pushed for FDA’s approval.)
Drug companies reflexively oppose lower drug prices, so of course they reflexively oppose imports from Canada. A statement from their trade association said they were “considering all options for preventing this policy from harming patients.”
If you wonder how patients could be harmed by lower drug prices, feel free to ask the Pharmaceutical Research and Manufacturers of America. Another question too: Ask if they could please, please, please cut down on those commercials (or better yet, just end them).