

SUBSCRIBE TO OUR FREE NEWSLETTER
Daily news & progressive opinion—funded by the people, not the corporations—delivered straight to your inbox.
5
#000000
#FFFFFF
To donate by check, phone, or other method, see our More Ways to Give page.
Daily news & progressive opinion—funded by the people, not the corporations—delivered straight to your inbox.

“This is not a grant reform—it is a blueprint for a spoils system applied to federal science funding."
An environmental watchdog group is calling on the White House Office of Management and Budget to withdraw a proposal that it said will give President Donald Trump and his allies unchecked power to control over a trillion dollars worth of federal grants.
Monday marked the end of the public comment period for a proposal from the OMB, spearheaded by Project 2025 architect Russell Vought and issued in late May, that would require all discretionary federal grants to “demonstrably advance the president’s policy priorities.”
As Elizabeth Kolbert explained in The New Yorker:
It would replace the current guidance for signing off on government grants, which generally leaves the task to civil servants and peer-review panels.
Instead, the final say would go to political appointees. All discretionary awards from the federal government would have to be assessed by senior administration officials, who could deny them on the [grounds] that they didn’t fit the President’s agenda. Grants could also be terminated at any time for the same reason.
The rules would affect hundreds of billions of dollars in funding disbursed by agencies ranging from the National Endowment for the Arts to the Transportation Department, to pay for everything from local dance performances to massive infrastructure projects.
Public Employees for Environmental Responsibility (PEER) filed a formal comment on Monday urging the OMB to withdraw the proposal.
"The scale of what is proposed is staggering," the group said. "This rule would institutionalize corruption and cronyism in the distribution of over a trillion dollars in annual federal funds."
The comment noted the proposal's language forbidding political appointees from deferring to peer review, which the group said will lead grants to be awarded based on ideological conformity rather than scientific merit.
"This language makes clear that the rule's purpose is not to add accountability over expert review but to replace expert judgment with political judgment entirely," the comment says. "Researchers would learn quickly to propose only work likely to survive ideological screening, while federal program officers, many of whom are being stripped of civil service protections, would face pressure to recommend or approve grants to preserve their jobs. "
“This would corrupt scientific judgment at every level of the process,” it adds, noting the Trump administration’s concerted effort to strip away funding for research on health and environmental issues that conflict with his political agenda, including climate science, vaccine safety, chemical safety, and emerging infectious diseases.
Since last year, the administration has terminated or frozen nearly 8,000 research grants and has effectively slashed the budget of the National Science Foundation by refusing to disburse funds appropriated by Congress. The agency is on track to issue the fewest grants in more than half a century, according to a report last month from Grant Witness.
The proposal would also allow agency heads to keep grants from being posted publicly whenever they determine that doing so would be contrary to the "national interest," which the rule does not define.
PEER said this change "permits agencies to offer grants by invitation only among preferred recipients with no requirement to explain or justify the determination."
The group pointed to the Trump administration’s pattern of directing no-bid contracts to the president’s family, friends, and supporters.
Trump megadonor and former Department of Government Efficiency (DOGE) head Elon Musk, the comment notes, was allowed to oversee the cancellation of the contracts for numerous vendors while never touching any of the more than $19 billion his businesses held in federal contracts.
“This is not a grant reform—it is a blueprint for a spoils system applied to federal science funding,” said Tim Whitehouse, executive director of PEER.
PEER's comment is one of nearly 342,000 OMB has received about the proposal in just over a month, of which 52,000 are publicly posted. The office is hoping to finalize the proposal by October 1 and has denied requests from watchdog organizations to extend the public comment period.
If that happens, Whitehouse has said it would upend the systems of accountability and transparency for scientific funding that have been in place for decades.
“Grant money has historically been distributed through programs authorized by Congress using statutory, regulatory, formula-based, or competitive criteria rather than direct tests of political loyalty,” added Whitehouse. “Placing all scientific research funding under the unreviewable discretion of political appointees is not an administrative reform; it is a recipe for corruption on a scale not seen even in this administration.”

Some of the satellites "would be the brightest ever in orbit, with damaging consequences for dark skies on Earth," said the European Southern Observatory.
European astronomers on Wednesday urged the US Federal Communications Commission to block a plan led by SpaceX CEO Elon Musk to launch a total of 1.7 million satellites into the Earth's orbit, warning that the use of so many extremely bright satellites—partially to support artificial intelligence data centers—would have “devastating consequences for astronomy.”
SpaceX's Starlink telecommunications program has already rapidly increased the number of satellites orbiting the Earth, with the total now exceeding 14,000 since 2019.
Now the space exploration company led by Musk—a former special government employee under the Trump administration—has plans to send 1 million more satellites into space, which would "significantly alter the appearance of the sky," according to a new study by the European Southern Observatory (ESO).
Scientists found that 100,000 is the maximum number of satellites—ones that are faint enough to be invisible to the naked eye—that can orbit the Earth in order to allow astronomers to continue observing the sky with modern telescopes.
In addition to Musk's launches, the US startup Reflect Orbital has proposed launching a constellation of 50,000 "very large mirror-like satellites to provide sunlight at night," said ESO.
"These satellites would be the brightest ever in orbit, with damaging consequences for dark skies on Earth," said the observatory. "Seen from within a reflected beam, the satellite delivering sunlight would appear four times brighter than the full Moon. Even if no satellite points its beam directly at an observer, each would be as bright as the planet Venus, the ‘morning star.' From a light-polluted city, like Munich, Germany, these hundreds of satellites would be the only ‘stars’ visible in the night sky."
The startup E-Space and two Chinese constellations, CTC-1 and 2, would also add hundreds of thousands of satellites into orbit.
The companies' satellite project could hinder scientists' ability to observe far-away galaxies, Earth-like planets near other stars, and asteroids that could potentially endanger the planet.
"Satellites, illuminated by the sun, are much brighter than distant galaxies. When a satellite crosses what we observe, it makes a bright streak on our image, zapping whatever is behind it," said ESO astronomer Olivier Hainaut, who led the study.
Hainaut noted that the planned launches could have economic and ecological impacts on the planet and humankind as well as harming astronomy.
Extreme light pollution from the bright satellites could disrupt people's biological clocks and ecosystems across the planet, and the satellites could also directly impact air quality due to the numerous launches required to send them into space and the "atmospheric pollution caused as they burn up on reentry at the end of life."
ESO conducted the research as the FCC considers applications from SpaceX and Reflect Orbital regarding the satellite launches
“The FCC received over 1800 comments regarding Reflect Orbital and nearly 1,500 comments on the application by SpaceX,” said ESO institutional affairs officer Betty Kioko. “The ball is now in the FCC’s court, and we wait to see the determinations they make on both filings. For optical astronomy, this is an existential threat, and we hope that the regulators will share that view.”

Late last week the White House announced plans for a major tightening of political control over research grants; instead of relying on the advice of expert panels as to which research should be funded, it will defer to political appointees.
There are moments when it feels like the president’s attention (as occasionally happens when we age) just keeps getting narrower and narrower—the things he really cares about (arch, reflecting pool, Kennedy Center, gilded horse statues) are all within a few miles of his home. He can barely be bothered to stay interested in the war he started in Iran; he’s more concerned with giving pretend tours of his imaginary ballroom. (“You come in, you have cocktails,” he explained to his daughter in law, interviewing him for Fox in true dear-leader fashion. “They they go through the door, in for dinner.”)
But the momentum behind the truly dangerous Project 2025 reordering of our society continues apace, even if—without Elon Musk to give it a face—we aren’t noticing. Late last week the White House announced plans for a major tightening of political control over research grants. Instead of relying on the advice of expert panels as to which research should be funded, as Kevin Bogardus explains:
One or more senior political appointees designated by their agency head must conduct “a pre-issuance review” of all discretionary grants, making sure they follow several principles, including to “demonstrably advance the President’s policy priorities.”
Since I enjoy making up new words (though surely someone has beaten me to this?) I’m going to call it “scilencing.”
The danger inherent in this should be entirely obvious. Jeff Mervis at Science interviewed a number of observers:
“What OMB [Office of Management and Budget] is proposing is not a reform of grants management,” Elizabeth Ginexi, a former program officer at the National Institutes of Health (NIH), writes in a Substack post. “It is a vehicle for complete political control of science… over every stage of the federal science funding lifecycle.” Representative Zoe Lofgren (D-Calif.), a leading critic of the Trump administration’s research policies, calls the proposal “a dystopian move that would destroy what remains of merit-based review.”
This would be a bad idea in a reason-based administration. In one that believes medieval nonsense about public health and that is eager to deregulate chemicals and end efforts to clean the air, it’s downright lethal.
And there is no doubt where the impulse really originated. The science the Trump administration really hates is climate science, because it threatens the “energy dominance” that the White House has made its basic foreign and economic policy, not to mention the profits of the fossil fuel industry that has been such an attentive donor. It’s not the first time that GOP administrations have tried to stymie climate science. Everyone remembers James Hansen’s crucial 1988 congressional testimony that global warming was underway; fewer recall that when he returned to Congress the next year the White House tried to rewrite and soften the conclusions in his testimony. That was under George H.W. Bush; under his son, in 2006, the White House tried again to rein him in. As he told Andy Revkin, NASA officials
ordered the public affairs staff to review his coming lectures, papers, postings on the Goddard Web site, and requests for interviews from journalists.
Dr. Hansen said he would ignore the restrictions. “They feel their job is to be this censor of information going out to the public,” he said.
Hansen was crucial enough—the Paul Revere of climate change—and senior enough that he was able to keep working and speaking. And the scientific research money kept more or less flowing. But now, in this new bureaucratic play, the Office of Management and Budget is trying to make sure that such independence (the single most obvious requirement for scientific advance) is a thing of the past. As John Timmer wrote at Ars Technica:
The result is a horror show for US science research. Not only is peer review made a secondary consideration, but the new rules would allow any federal agency to cancel any grant at any time based on the vague assertion that it isn’t in the “national interest.” The document would also ban any grants on a number of culture war topics, limit international collaborations, and block spending on things like publishing papers and attending conferences.
It is, in short, a recipe for how the government can finish the job of crippling American science.
This is not yet a done deal. There is a 45-day comment period for letting the government know what you think of their plan, and 41 of those days remain. Here’s the place to have your say.
I’m not, I must say, convinced they’ll pay great attention to the comments, so it’s also crucial to be letting your congresspeople know what you think about this attack on science. Congress has so far been able to save at least some of the things Russell Vought has sought to kill: indeed, word came this week that the NOAA budget will include money to keep the carbon dioxide observatory at Mauna Loa (aka the world’s most important scientific instrument) up and running. That’s a direct result of Congress hearing outcry, so let’s keep it up.
Remind them that real leaders actually want to know what science can tell them—case in point, the remarkable new movie, Pressure, which tells the story of how General Eisenhower listened to the new and unorthodox science of meteorology to guide his D-Day decision making (95% on Rotten Tomatoes, for those of you who like numbers).
That changes on this scale are possible is precisely what terrifies the fossil fuel industry, and in turn the Trump administration.
The good news, I suppose, is that on climate and energy the cat has largely escaped the bag. We do know what the problem is, even if the ramifications become more dire with each passing week. (Here’s a somewhat terrifying update on the prospects for this year’s wildfire season; meanwhile, Tom Harris has the new numbers on Antarctic melt.). And we know where the solution lies. Indeed, it too comes into clearer focus with each passing week. As I wrote earlier this year, the action in the next few years is going to be about batteries, and boy is that proving true. Bloomberg confirmed last month that 2025 was the first year the world installed more than a hundred gigawatts of battery storage, up 48% from the year before, and expected to grow another 46% this year.
South Australia held a big auction last month for “firm supply” across the territory’s electric grid. This is supposed to be the last place where fossil fuel is superior: always-on power. But all the low bids came from companies that wanted to (and now will) install big batteries. As Giles Parkinson reported:
It is yet another sign of the growing dominance of battery storage technology in Australia’s main grids (and off grid).
Big batteries have dominated other long duration storage tenders, particularly in NSW [New South Wales], were it has sidelined pumped hydro projects, and battery storage has been steadily sending gas peakers to the sidelines, particularly in the demand peaks they used to dominate.
Indeed, Australia is emerging as the test case for just how fast and furiously you can switch a grid to clean renewables. Even as its government continues to mine huge amounts of coal to send abroad, it’s providing a generous domestic subsidy for Aussies who want to put smaller batteries in their homes. And that, in turn, is underwriting a revolution on the grid. As Adam Morton and Petra Stock wrote this past week:
Nearly 60% of the household-scale battery capacity installed across almost 200 other countries this financial year will be in the southern continent, according to a recent analysis. Since July, about 415,000 have been connected—roughly 1 unit for every 25 Australian homes.
Previously, power prices would rocket in the evenings as gas-fired power—the most expensive form of energy generation on the Australian grid—was turned on to meet peak demand. With solar and wind now providing nearly half the electricity, and coal-fired power plants gradually closing, gas has been used to fill gaps after the sun sets.
But batteries are increasingly taking over that role. Total gas-fired generation was 24% lower across three months this summer compared with the year before. Tennant Reed, the climate change and energy director with the Australian Industry Group, representing more than 60,000 businesses, says it has “completely changed how electricity prices are formed.”
I hope you’ll go back and read the sentence I italicized in the last paragraph: the use of gas to create electricity dropped 23% in a year. This is much like what’s happened in California, where Mark Jacobson reports that the world’s fourth largest economy is using 60% less gas to produce electricity than it did three years ago. That changes on this scale are possible is precisely what terrifies the fossil fuel industry, and in turn the Trump administration.
Beginning one month from tomorrow, Australians, whether they have solar panels or batteries or none of the above, will get three free hours of electricity every afternoon from noon to 3:00 pm.
And the possibilities are everywhere. Canary Media’s Julian Spector wrote last week, a new global report shows that these so-called “firm renewables” (wind and sun coupled with batteries)
“has crossed the threshold of cost competitiveness with new fossil fuel generation,” in areas with plenty of sun or wind. “The central question is no longer whether firm renewables can compete on cost, but how quickly the structural conditions needed to realise their potential can be put in place across the diversity of markets and institutional contexts prevailing globally.”
China sets the bar with its shockingly low cost of firm renewables today.
IRENA [International Renewable Energy Agency] looked at 252 solar projects that went online there in 2024 and found that many of them could be augmented with extra solar capacity and batteries to deliver power cheaper than the $100-per-megawatt-hour benchmark for new gas-fired plants. Almost all the modeled solar-battery plants could beat that cost for firm clean power 90% of the time; even at the higher reliability threshold of 99%, nearly half the projects remained competitive, and the lowest cost was $46 per megawatt-hour.
And would any of this be, I don’t know, politically popular?
Beginning one month from tomorrow, Australians, whether they have solar panels or batteries or none of the above, will get three free hours of electricity every afternoon from noon to 3:00 pm. If you want to know why our government needs to shut up scientists and ward off engineers, that’s why.
Oh, they’re also trying to shut down the world’s central archive of disasters, which lets us learn from the past. I predict that will not slow the pace of trouble.

UM research Dr. Danhao Wan reportedly committed suicide after being questioned by federal authorities, revealing a broader pattern of political discrimination.
On April 17, CODEPINK and the local University of Michigan community gathered to hold a vigil in honor of UM researcher Dr. Danhao Wan on the one-month anniversary of his death. According to reports, Dr. Wang died after jumping from an upper floor of the G.G. Brown Building on North Campus, shortly after being targeted and questioned by federal authorities.
Over 30 members of the local community attended the vigil, bringing candles and flowers. They joined in a traditional Chinese bowing ceremony. During the vigil, CODEPINK and US Peace Council member Bob McMurray spoke to the crowd: “Tonight, I want us to remember there is a Mom and Dad mourning the loss of their son; there are people here in the university research community feeling his absence every day; and we, as the human family, have lost a brother.”
For weeks, Dr. Wang’s death went uncovered by the media. By the time it hit the news, the Chinese Consulate in Chicago had already confirmed the incident as a suicide and demanded an investigation of the “unwarranted interrogations and harassment of Chinese students and scholars.”
This is not the first time a Chinese scholar has been targeted at the University of Michigan; it is part of a broader pattern of political discrimination. In the last year, five Chinese scholars have been accused of various crimes, detained for months on end, and ultimately deported after the quiet dismissal of their cases due to a lack of evidence.
When individuals like Dr. Wang are targeted, it is not only their livelihoods that are threatened, but the very purpose and meaning they have built their lives around.
This discrimination is not new. In 2018, the Trump administration launched the China Initiative, a deeply flawed and racially biased program that targeted Chinese and Chinese Americans for “suspected espionage.” More often than not, federal authorities targeted individuals with no evidence of wrongdoing—simply for their identity. As a result, a new climate of suspicion and fear took root across academia. Though few convictions were made, many Chinese scholars suffered permanent professional and personal harm. They began to self-censor, withdraw from collaborations, or leave the United States entirely. For them, the US was no longer safe.
Although the China Initiative was formally ended under the Biden administration due to widespread criticism of its racial bias, its underlying logic has not disappeared. Instead, it has evolved into a broader atmosphere of suspicion directed at Chinese scholars, particularly in fields tied to advanced technology and science. At the University of Michigan, this pattern is especially visible.
Take the case of Dr. Chengxuan Han, a Chinese PhD student who was arrested for mailing roundworms commonly used in biological research. In most academic contexts, such an error would result in a minor administrative penalty. Instead, she was jailed for months and subjected to a full criminal prosecution. This outcome was wildly disproportionate to the alleged offense and one that effectively ended her academic trajectory.
Another scholar, Dr. Yunqing Jian, was accused of "agricultural terrorism” for breaking protocol and shipping materials to the US without the proper paperwork. Renowned biologists refuted this claim, saying it was impossible to use Fusarium graminearum, the fungus Dr. Jian studied, as a bioterrorist weapon. In the world of research deadlines and red tape, scholars say it's typical to try to streamline research by acquiring your own materials, even if that means skipping some paperwork. Dr. Jian has spent years researching how to mitigate the harm caused to crops by Fusarium graminearum, which is native to North America. While she did break protocol, it is absurd to accuse her of weaponizing the fungus, especially without any evidence.
Similarly, the cases of UM scholars Xu Bai, Fengfan Zhang, and Zhiyong Zhang demonstrate how ordinary research practices were reframed as criminal acts merely because of the identity of the scholars. Even though charges against them were dropped and the cases dismissed, the damage had already been done.
The three scholars had spent months in jail awaiting their trial. In a letter, Zhiyong Zhang spoke of his confusion over the situation:
I like the research atmosphere in the University. I like the people here. They are kind and polite. I am living a happy life here. However, unfortunately and apparently, some people don't like us. They want to connect us with politics. But what is politics? I didn't know what politics is when I was 13 years old, at which age I decided to study biology. Now I am also confused about what politics is. It's so abstract. We didn't hurt anyone, and we don't want to hurt anyone, either. We just want to do research and find something that can benefit humanity. That makes me feel my life is meaningful, although I can not make much money.
Zhang decided to study biology because his grandfather and father were both diagnosed with Parkinson’s disease in their mid-30s: “I thought I could change to study neuroscience to cure the disease of my family and all the people who are suffering the pain from the disease… So this is what I am doing here.” At 32, he worries he will soon suffer the same fate.
Originally, the three scholars were informed by the University of Michigan that they had 30 days to pack and leave. Since they’d spent all their free time in the laboratory, they decided to use their last few weeks to visit the Grand Canyon. While there, the UM administration backtracked on their words, informing the scholars they had to leave immediately. At the airport, while attempting to return home, they were intercepted by Immigration and Customs Enforcement and arrested.
This was no coincidence. The UM administration not only provided the wrong information, but they also had terminated their SEVIS status, which gave them permission to live and study in the US, making them vulnerable to federal authorities at passport control.
The repeated pattern points to a system in which Chinese researchers are treated as potential threats merely on the basis of their identity—which is all a part of the larger campaign to paint China as an enemy of the United States.
Dr. Danhao Wang’s life and work stand in stark contrast to this narrative. An assistant research scientist in the University of Michigan’s College of Engineering, Dr. Wang dedicated his career to advancing semiconductor technology. His research focused on gallium nitride, a material critical to modern electronics and essential for improving the speed, efficiency, and energy consumption of devices ranging from smartphones to renewable technology systems.
He made significant contributions to understanding how these materials behave at the atomic level, correcting long-standing assumptions and helping to unlock new possibilities for high-performance electronics. His work also explored how next-generation semiconductors could remain stable under extreme electrical conditions, paving the way for more efficient energy systems and emerging technologies.
We must put increased pressure on the University of Michigan and other universities to do more to protect their international students.
The repercussions of this research are vast. Semiconductors with such high performance potential could potentially make the data center industry obsolete by enabling a smaller device to do what normally takes an entire facility. For the US, gallium nitride semiconductors are the key to significantly improving its high-power weapons systems, and China’s current dominance over the material is considered a looming threat. This is all part of the US preparation for war against China, and the ongoing arms race around strategic resources and technology.
It’s reported that Dr. Wang was planning to return to China in May and already had a job set up. This raises even more questions over the circumstances of his death, and many Michigan locals have begun calling for an independent investigation.
Like most scientists, Dr. Wang’s research stemmed from deep intellectual commitment and passion. Years of specialized training, long hours in the lab, and a singular focus on discovery defined his life’s work. When individuals like Dr. Wang are targeted, it is not only their livelihoods that are threatened, but the very purpose and meaning they have built their lives around.
His death is a profound tragedy. And while the full circumstances remain unclear, it occurred within an environment where Chinese scholars have repeatedly been subjected to intense surveillance and unfair targeting.
The broader political climate cannot be ignored. Increasingly, US policy and rhetoric have framed China as a primary geopolitical adversary, particularly in areas like technology and national security. This framing has filtered down into academic spaces, where international collaboration between the US and China is now essentially criminalized.
The Chinese Consulate in Chicago has criticized the US for “overstretching the concept of national security” and has called for a full investigation and accountability. These demands should not be dismissed.
There must be transparency around the circumstances leading to Dr. Wang’s death. There must also be concrete safeguards to prevent discriminatory investigations targeting international scholars. This includes stronger legal protections, clearer institutional accountability, and accessible mental health support for those under investigation.
Universities, in particular, have a responsibility to protect their students and researchers. The University of Michigan is clearly doing the opposite. They are not protecting their students; they are instead actively targeting them by aiding these discriminatory investigations, putting all international students at risk.
We must put increased pressure on the University of Michigan and other universities to do more to protect their international students, to preserve the integrity of academic research, to protect international collaboration, and to ensure that scientific progress is not undermined by federal discrimination. If institutions fail to act, the cost will not only be measured in lost careers but in lost knowledge, lost innovation, and lost lives.

The biggest threat isn’t scientific uncertainty, since there’s a considerable amount of scientific consensus that there is plastic in us. The biggest threat is weaponized uncertainty used to delay regulations.
“Microplastics are everywhere, and they’re harming us.”
“Actually, maybe not.”
“Hold on, that study might be flawed.”
“Bombshell… the whole field is in doubt.”
The headline isn’t “microplastics in people might be wrong,” but rather “quantifying microplastics in human samples is challenging, and the science is evolving in the right direction.”
If you’ve been hearing about microplastics recently, you may have been getting whiplash from the headlines. But you shouldn’t be.
Because this is what science looks like when it’s working: Researchers test new ideas and challenge each other’s methods. This helps refine what we know. What isn’t supposed to happen is a normal, healthy, scientific process getting manipulated into a dramatic storyline about a fictional scandal—a story that can leave the public confused.
For over two decades, we’ve studied plastic pollution in the ocean. Scientists started describing the accumulation zones of plastic in the subtropical gyres, the places where wind and water currents concentrate floating debris. The research pointed to a truth that was complicated but clear: Most of the pieces are tiny, fragmented plastic—microplastics—along with some larger marine debris, like fishing gear.
But the media put a spin on it, and gave the world a simpler picture: a floating island of trash, “twice the size of Texas.” Some even called this a “garbage patch” you could supposedly walk on. People cried, “Why can’t I see it on Google Maps?” Some wondered if the US should plant a flag, and a handful of naive entrepreneurs fabricated fantastic ocean cleanup contraptions.
It was dramatic. Word spread. But eventually, it backfired.
All those who went looking for an island, didn’t find one. Instead they concluded, “It’s more like smog than a landfill,” and some pointed out, “Maybe it was exaggerated and the world had been duped.”
The pattern—one that goes oversimplify, sensationalize, backlash, dismissal—can drain urgency from a real crisis. Misinformation gets the headline. This gets repeated, as we’ve seen before in other environmental debates, such as the hole in the ozone layer, or climate change. The same thing is unfolding now with microplastics and human health.
The recent article in The Guardian that sparked this debate focuses on a real issue. In our research studying microplastics in the environment and animal studies, measuring micro- and nanoplastics in human tissue is incredibly hard. It is particularly difficult when researchers are looking for very small particle sizes, where laboratory contamination from airborne sources becomes harder to rule out. This is especially the case in human tissue.
Microplastics are not like other contaminants, such as lead in water, where you can measure parts per billion, and lean on decades of standardized instruments and test methods. Plastics come in many polymers, sizes, and shapes. Nanoplastics behave differently than microplastics. And plastic is everywhere, meaning background contamination is always a risk. This is sometimes called the “pig pen effect”—it is a challenge to study a material that is so widespread.
The Guardian article is not a devastating blow. It’s a scientific debate around specific methods in a research field that is rapidly improving.
The headline isn’t “microplastics in people might be wrong,” but rather “quantifying microplastics in human samples is challenging, and the science is evolving in the right direction.”
That difference matters. If the public hears “doubt cast,” then it translates it as “maybe plastic pollution isn’t really there or not that bad.” The question is, does it hold up across methods, across labs, across time?
So what has science taught us?
The biggest threat here isn’t scientific uncertainty, since there’s a considerable amount of scientific consensus that there is plastic in us. The biggest threat is weaponized uncertainty.
Environmental health has a predictable plot—when evidence starts piling up that a pollutant is harmful, a well-funded countermovement doesn’t always try to prove it’s safe. On the contrary, it tries to prove that the science is messy, uncertain, and “we need more data.”.
We’re not asking journalists to avoid urgency. Plastic pollution is urgent. Certain phrases, however, may signal that you’re being pulled into a pattern of mythmaking.
The industry has a playbook with favorite phrases, such as: “not conclusive,” “uncertain,” “scientists disagree,” “lack of consensus.” Disagreement in science is healthy. However, this (very routine) component of science can also become a winning political strategy used against science and public policy. Casting doubt can delay regulation.
Naomi Oreskes writes in Merchants of Doubt, “The industry had realized you could create the impression of controversy simply by asking questions.” That’s why our concern isn’t that researchers are debating methods. Our concern is that sensational headlines can warp debate, and give merchants of doubt an opportunity to skew public perception.
We’re not asking journalists to avoid urgency. Plastic pollution is urgent. Certain phrases, however, may signal that you’re being pulled into a pattern of mythmaking, such as “bombshell,” or “debunked,” when what’s really happening is refinement. Those phrases shock and entertain, but do little to foster understanding.
What we actually need next is for the microplastics field to keep growing. Researchers across the board—from those that think studies are exaggerated to those that stand behind their research findings—are making calls for better lab protocols, contamination controls, reporting requirements, and inter-lab studies to validate results. These are unglamorous, but they’re what solidify early research findings into trusted science. A first-of-its-kind finding of plastic somewhere in the human body shouldn’t be framed like the final truth. It should be heralded as the beginning of a more complete picture.

His new dietary guidelines promoting saturated fats are a recipe for disaster, and a heart attack.
Fat is now phat, at least according to Robert F. Kennedy Jr.
When President Donald Trump’s Health and Human Services (HHS) secretary unveiled new federal dietary guidelines this January, he declared: “We are ending the war on saturated fats.” Seconding Kennedy was Food and Drug Administration Commissioner Marty Makary, who promised that children and schools will no longer need to “tiptoe” around fat.
Kennedy’s exaltation of fat comes complete with a new upside-down guidelines pyramid where a thick cut of steak and a wedge of cheese share top billing with fruit and vegetables. This prime placement of a prime cut is the strongest endorsement for consuming red meat since the government first issued dietary guidelines in 1980.
The endorsement reverses decades of advisories, which the US Department of Agriculture (USDA) and HHS jointly issue every five years, to limit red meat consumption issued under both Democratic and Republican administrations given the strong evidence that eating less of it lowers the risk of cardiovascular disease. Multiple studies over the last decade have linked red and processed meats not only to cardiovascular disease, but also to colon polyps, colorectal cancer, diabetes, diverticulosis, pneumonia, and even premature death.
Given the scientific evidence, we should intensify the war against saturated fats, not call it off.
The new dietary guidelines even contradict those issued under the first Trump administration just five years ago, warning Americans not to eat too much saturated fat. “There is little room,” those guidelines stated, “to include additional saturated fat in a healthy dietary pattern.” A significant percentage of saturated fat comes from red meat. Americans, who account for only 4% of the people on the planet, consume 21% of the world’s beef.
Kennedy’s fatmania even extends to beef tallow and butter, which the new pyramid identifies—along with olive oil—as “healthy fats” for cooking. In fact, beef tallow is 50% saturated fat. Butter is nearly 70%. Olive oil, meanwhile, is just 14% saturated fat and is, indeed, healthy.
This rendering of recommended fats muddles a message that could have been stunningly refreshing, given the Trump administration’s penchant for meddling with science. Some of the new pyramid’s recommendations were applauded by mainstream health advocacy groups, particularly one advising Americans to consume no more than 10 grams of added sugar per meal and others, as Kennedy pointed out, calling for people to “prioritize whole, nutrient-dense foods—protein, dairy, vegetables, fruits, healthy fats, and whole grains—and dramatically reduce highly processed foods.”
But such wholesomeness could easily be wasted if Americans increase their meat consumption. That would not, as Kennedy professes, make America healthy again. Given the scientific evidence, we should intensify the war against saturated fats, not call it off.
The 420-page report by the Dietary Guidelines Advisory Committee prepared in 2024 for the USDA and HHS found that more than 80% of Americans consume more than the recommended daily limit of saturated fat, which is about 20 grams—10% of a 2,000 calorie-per-day diet. The report concluded that replacing butter with plant-based oils and spreads higher in unsaturated fat is associated with lower cardiovascular disease risk and eating plant-based foods instead of meat is “associated with favorable cardiovascular outcomes.”
A March 2025 peer-reviewed study in JAMA Internal Medicine came to a similar conclusion. It found that eating more butter was associated with a higher risk of cardiovascular disease and cancer. Using plant-based oils instead of butter, the researcher found, was associated with a 17% lower risk of death. Such a reduction in mortality, according to study co-author Dr. Daniel Wang, means “a substantial number of deaths from cancer or from other chronic diseases … could be prevented” by replacing butter with such plant-based oils as soybean or olive oil.
What does a “substantial” number of deaths look like? Heart disease is the No. 1 killer in the United States, and heart disease and stroke kill more people than all cancers and accidents combined. The annual number of American deaths tied to cardiovascular disease is creeping toward the million mark. According to the American Heart Association (AHA), it killed more than 940,000 people in 2022.
Over the next 25 years, AHA projects that the incidence of high blood pressure among adults will increase from 50% today to 61%, obesity rates will jump from 43% to 60% and diabetes will afflict nearly 27% of Americans compared to 16% today. Reducing mortality by 17% for those and other related health problems would go a long way to make Americans healthier.
A good place to begin reducing food-related mortality is by cutting highly processed foods out of the American diet. That would require a drastic change in eating habits for a lot of people. A July 2022 study found that nearly 60% of calories in the average American diet comes from ultra-processed foods, which have been linked to cancer, cardiovascular disease, depression, diabetes, and obesity.
One of the main culprits is fast food. A January 2025 study of the six most popular fast-food chains in the country—Chick-fil-A, Domino’s Pizza, McDonald’s, Starbucks, Subway and Taco Bell—found that 85% of their menu items were ultra-processed. And, according to a 2018 study, more than a third of US adults dine at a fast-food chain on any given day, including nearly half of those aged 20 to 39.
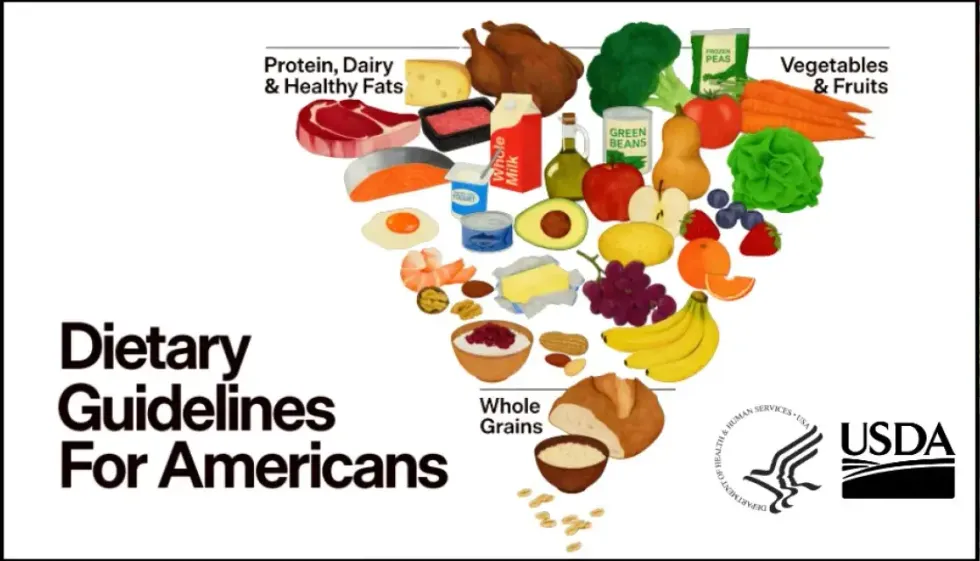 The new federal dietary guidelines reverse decades of advisories that recommended limiting red meat consumption. (Illustration: HHS/USDA)
The new federal dietary guidelines reverse decades of advisories that recommended limiting red meat consumption. (Illustration: HHS/USDA)
Our overreliance on fast food presents a huge conundrum. US food systems are structured in a way that it is unlikely you can tell people to cut processed foods and eat more meat at the same time. Hamburgers and processed deli meat are among the main ways Americans consume red meat. And given the blizzard of TV ads for junk food and fast-food joints, which have proliferated across the country and especially in low-income food deserts—it is also unlikely that many people will use the new guidelines to comb through their local grocer’s meat department for the leanest (and often most expensive) cut of beef.
According to the University of Connecticut’s Rudd Center for Food Policy and Health, food, beverage, and restaurant companies spend $14 billion a year on advertising in the United States. More than 80% of those ad buys are for fast food, sugary drinks, candy, and unhealthy snacks. That $14 billion is also 10 times more than the $1.4 billion fiscal year 2024 budget for chronic disease and health promotion at the Centers for Disease Control and Prevention. And don’t expect the CDC to get into an arms race with junk food advertisers any time soon. Kennedy slashed the CDC staff by more than 25%, from 13,500 to below 10,000.
All of this adds up to the probability that Americans will see the new guidelines’ recommendation to eat red meat as a green light to gorge on even more burgers and other fast-food, ultra-processed meat.
The new guidelines’ green light for consuming red meat and saturated fats is particularly vexing given the guidelines produced five years ago during Trump’s first term did not promote them. Why the about-face?
During the run-up to Trump’s second term, the agribusiness industry went into overdrive to install Trump in the White House and more Republicans in Congress. In 2016, agribusinesses gave Trump $4.6 million for his campaign, nearly double what it gave Hillary Clinton. But in 2024, they gave Trump $24.2 million, five times what it gave Kamala Harris. Agribusinesses also donated $1 million to Kennedy’s failed 2024 campaign, making him the fourth-biggest recipient among all presidential candidates during that election cycle.
Robert F. Kennedy Jr. is nowhere near making America healthy again by declaring in his new food pyramid that red meat is as healthy as broccoli, tomatoes, and beans.
Despite claiming he wanted dietary guidelines “free from ideological bias, institutional conflicts, or predetermined conclusions,” Kennedy rejected the recommendations of the Dietary Guidelines Advisory Committee and turned over the nation’s dietary data to 9 review authors, at least 6 of whom had financial ties to the beef, dairy, infant-formula, or weight-loss industry.
Three of them have received either research grant funding, honoraria, or consulting fees from the National Cattlemen’s Beef Association, which is known for funding dubious research downplaying or dismissing independent scientific findings that show read meat to be threat to public health and the environment. In 2024, the trade group gave nearly all of its $1.1 million in campaign contributions to Republican committees and candidates.
Kim Brackett, an Idaho rancher and vice president of the beef industry trade group, hailed the new guidelines, claiming “it is easy to incorporate beef into a balanced, heart-healthy diet.”
Perhaps, but the grim reality is most Americans do not follow a balanced, heart-healthy diet. Four out of five of us are already consuming more than the recommended daily limit of saturated fat and we are well on our way to a 60% obesity rate.
So, Robert F. Kennedy Jr. is nowhere near making America healthy again by declaring in his new food pyramid that red meat is as healthy as broccoli, tomatoes, and beans. Beholden to Big Beef, he is driving us full speed ahead on the road to a collective heart attack.
This article first appeared at the Money Trail blog and is reposted here at Common Dreams with permission.

Cancer and other noncommunicable diseases remain chronically underfunded in low- and middle-income countries. This neglect is not only unjust; it is destabilizing.
As the year draws to a close, I find myself thinking about what lingers after the headlines fade.
I am thinking about the corridors of a cancer conference in Tunisia, where doctors, nurses, scientists, students, and patients from across Africa gathered with a shared purpose: to reduce the burden of cancer in places too often overlooked. In conversation after conversation, I heard stories of ingenuity and quiet endurance; clinicians delivering chemotherapy with limited supplies, researchers building cancer registries on borrowed computers, patients selling what little they own to stay alive.
One young oncologist from Rwanda told me he is learning to speak differently with his patients about cancer. Not just about treatment protocols, but about fear, dignity, and hope. He explained how language itself can heal, how empathy can ease suffering even when resources are scarce. I called him the prophet—not because he predicted outcomes, but because he understood that healing begins with trust.
A breast cancer survivor from Gaza spoke of women forced to leave home in search of treatment, only to face drug shortages and fractured care across borders. Their struggle is not only against disease, but against politics and geography that interrupt therapy and shorten lives.
If the year ahead is to mean progress, it will depend on whether we choose to align wealth with wisdom and urgency with solidarity.
These stories stayed with me when I returned home; and when I read, almost casually, about tens of millions of dollars spent to influence a single political race in New York City. I could not stop doing the math. How many nurses could that money train? How many pathology labs could it equip? How many mothers could it help live long enough to watch their children grow?
We live in a moment when the science to dramatically reduce cancer and other noncommunicable diseases already exists. Prevention works. Diagnostics work. Treatment works. Yet survival remains a cruel lottery of birth. A child with leukemia in Boston, Heidelberg, or Tokyo has more than an 80% chance of survival. The same child in Kampala, Dhaka, Sana’a, or Gaza faces odds closer to 20%; not because science has failed, but because access has.
This inequity is not academic for me. I am living with stage IV cancer. My treatment is possible not because I am exceptional, but because of where I live. My ZIP code granted me specialists, hospitals, and medicines that millions of people around the world cannot access. In an era of breathtaking biomedical progress, this disparity is increasingly difficult to defend.
Meanwhile, vast sums continue to flow effortlessly toward political influence, luxury consumption, and fleeting spectacle; multimillion-dollar celebrations, couture collections, brief trips to the edge of space. Excess has always existed, and it always will. The question is not whether extravagance can be eliminated, but whether it must remain our highest expression of success.
History shows us another option. Coordinated global investment transformed the trajectory of HIV, tuberculosis, and malaria. Millions of lives were saved not because the science was perfect, but because resources were mobilized with urgency and moral clarity. When funding aligns with purpose, outcomes change—quickly and dramatically.
Yet cancer and other noncommunicable diseases, now responsible for most deaths worldwide, remain chronically underfunded in low- and middle-income countries. This neglect is not only unjust; it is destabilizing. Untreated cancer weakens families, strains health systems, and erodes trust in institutions. The consequences ripple far beyond individual patients.
As the year ends, it is worth asking what our spending reveals about our values. Conferences like the one I attended in Tunisia are not only scientific gatherings; they are moral ones. They confront us with the gap between what is possible and what we choose to prioritize.
We live in a world of abundance and absence, sometimes within the same news cycle. One story celebrates money deployed for influence; another recounts lives lost for lack of basic medicine. These are not separate realities. They are the result of collective choices.
As the new year begins, we will make choices—about budgets, priorities, and what we choose to celebrate. Those choices will determine who receives care and who waits, who lives and who is left behind. Science has already shown us what is possible. If the year ahead is to mean progress, it will depend on whether we choose to align wealth with wisdom and urgency with solidarity, deciding, at last, that saving lives deserves the same resolve we devote to influence, attention, and prestige.

Libraries are indispensable not only for climate and informational literacy but also as valuable hubs for creating community solutions to our planet’s most pressing problems.
If you’re a parent, caregiver, or family member hoping to save a few bucks this holiday season due to our country’s affordability crisis, you’re not alone.
As a lifelong educator and author who practically grew up in libraries, I can offer you a great tip: Skip the malls this season and take kids to the local library. Within their walls awaits an exciting world of lessons and self-empowerment for your child. They can borrow books or even movies for free. More than that, libraries have become ground zero for climate change education and serve as essential hubs for community resilience and civic engagement.
As a former public school teacher, a professor, and the author of two books on climate change and environmental justice education, public libraries were essential to my success. Growing up, I was that kid who was friends with the librarian. As an introverted student, the public library and school library were places of refuge where I found joy in the world of books. Memories of friendly librarians who encouraged my insatiable curiosity and quest for knowledge are among the many reasons I became an educator.
Here are three ways to get the most out of your local library:
I always tell my students that you don’t need the newest “gadgets” to make a meaningful impact. I know that many parents, caregivers, and families are struggling with inflation and the rising costs of goods, especially as the holidays approach. One of the easiest remedies is to repair rather than replace, which is a climate change solution because it reduces waste sent to landfills.
Instead of buying more, fixing damaged or broken belongings like clothes, furniture, and electronics can teach new skills, foster self-reliance, and build connections with family or the community. For example, some meaningful childhood memories were fixing my toys with my dad and learning how to use tools, which sparked my interest in STEM education and sustainability.
Instead of asking what to buy kids, think about what new information and skills they can be taught.
Many public libraries, makerspaces, and city sustainability offices offer “Repair Cafes,” or “Fix-It Clinics,” that feature hands-on and intergenerational events where people can bring in their broken items, and repair coaches provide instructions on how to fix them. Events have occurred in Los Angeles, Washington, DC, Albuquerque, New York, and San Diego. See if any events are happening in your community. Additionally, if you’re already handy and have repair skills, libraries around the world offer tool lending programs. You can search for a library near you to borrow a kit.
Learners of all ages can take action on climate change and explore their backyard, community, or neighborhood. Libraries also serve as public Earth observatories. To be a neighborhood or backyard scientist, you can also visit a library.
Neighborhood science, also known as Citizen Science or Community Science, comes alive when ordinary people of any age gather scientific information locally and share it with the global scientific community. For example, with a library card, you can check out a citizen science kit that has all of the necessary tools to explore biodiversity, observe cloud patterns, and monitor air quality.
Libraries around the country have citizen science kits, including the Los Angeles Public Library, the Maricopa County Library District, the Pima County Public Library, the Morgantown Public Library System, the Edwardsville Public Library, and the Longwood Public Library. Families and caregivers can even practice their skills and gear up to participate in Audubon’s legendary Christmas Bird Count that occurs every December, and is the nation’s longest-running community science bird count. Libraries have stepped in to fill a critical gap in climate literacy and community resilience during the climate emergency. However, libraries are also being targeted by the Trump administration.
The Trump administration has a clearly established anti-information agenda. The long and expanding list includes book bans and information censorship; attacks on cultural and educational institutions that teach the truth about American history; attempts to eliminate the Institute of Museum and Library Services, which provides significant funding to libraries nationwide; and firing the librarian of Congress, the nation’s top librarian. Librarians at federally operated presidential libraries have been fired, like at the John F. Kennedy Presidential Library and Museum in Boston.
Funding public libraries also helps finance city and county sustainability efforts. Libraries are climate resilience hubs, and libraries across the country serve as community cooling centers amid rising temperatures associated with climate change. Amid the heatwaves that have impacted Los Angeles over the past several years, I’ve visited some Los Angeles Public Library locations for a reprieve from triple-digit heat.
Libraries are also disaster recovery hubs. As a result, climate action groups, fire departments, emergency management agencies, and local businesses can also rally to demonstrate the value of public libraries to the community’s sustainability plans. Advocacy groups can also lobby state and regional representatives. Libraries are indispensable not only for climate and informational literacy but also as valuable hubs for creating community solutions to our planet’s most pressing problems.
Instead of asking what to buy kids, think about what new information and skills they can be taught: The climate crisis needs more innovative, creative, and community-driven solutions, and libraries are primed to help.

The new denialism no longer bellows about hoaxes; it asks for more studies, more modelling, more consultations, always in the service of delay.
Belém promised a “COP of truth.” What unfolded was a courteous unravelling of ambition, as denialism left global climate action wobbling at the moment it needs steel.
As the Chair of the UK’s COP30 youth delegation, I realized within hours that this United Nations climate conference would be defined by its optics—not its outcomes. The venue teemed with political hopefuls more interested in cameras than commitments, and with a record 1,600 fossil fuel and 531 carbon-capture lobbyists, 1 in every 25 attendees served commercial interests.
Then came the negotiations, where delegates quietly diluted the science. References to the Intergovernmental Panel on Climate Change (IPCC), long regarded as the global lodestar of climate knowledge, were either softened into ambiguity or dropped altogether. Several companies went even further, trumpeting improvements in emissions intensity as if they were genuine reductions.
It was greenwashing par excellence, a polite fiction to excuse keeping emissions exactly where they are.
After the failures of COP29 and COP30, the process will only matter again if governments are finally pushed toward honesty and supported by tools that can hold them to it.
So it was no surprise when the negotiations titled toward erasure, governing not just the deal but the language that framed it. The term “fossil fuel” vanished from the final Belém Political Package, replaced with sweeping and unenforceable vows to renewables and adaptation funding.
We should have foreseen how settled climate science would be twisted and spun. After all, one investigation found more than 14,000 pieces of COP-related disinformation in just the three months before Belém. Much of it was generated by AI, including a widely shared fake video that showed the host city swallowed by floods.
This version of climate denialism reveals the moral credibility of climate action is being leveraged to keep emissions frozen in place. It no longer bellows about hoaxes, except by Donald Trump who has happily dragged America back into isolationism. In the diplomatic world it asks for more studies, more modelling, more consultations, always in the service of delay. It is denialism wearing the mask of governance, and it is far more corrosive than the loud bluff it replaced.
The timing could hardly be worse. The IPCC’s carbon budget for a 50% chance of staying below 1.5°C will vanish by 2029 if emissions continue at today’s pace. This is also the first year after the Global Stocktake that mandates governments to draft national plans that will set our course until 2030.
And what happens now determines the shape of the decisive decade. Crossing 1.5°C sharply raises the risk of irreversible cryosphere collapse—rapid ice loss in Antarctica and Greenland which will lock the world into meters of sea-level rise that imperil coastal megacities across every hemisphere. At 2°C, another billion people will face severe water scarcity—especially in the Global South where adaptation capacity is lowest and exposure is highest. This reality is why the deliberate sidelining of climate science is not just exasperating but catastrophic.
And COP30’s lone nod to honesty—the Declaration on Information Integrity—feels painfully thin. The declaration, which promises to counter climate falsehoods, was only signed by 12 countries. And with no sanctions or accountability, it is a gesture at truth in the exact moment truth needed teeth.
We need a global firewall for climate truth: binding rules for climate information, a UN body capable of verifying data with transparent AI, and legal duties on platforms to curb the algorithmic spread of lies. Climate inaction is becoming a matter of legal liability. That burden should fall equally on those who deliberately twist the science.
There must be a counterweight capable of tracing disinformation, naming the culprits of confusion, and dragging the debate back to the science that anchors it. Only then can we hope to restart global climate momentum. And in an irony worthy of our age, the technology that helped generate the mess—AI—may be the only thing sharp enough to cut through it.
According to Sachin Dev Duggal, Britain’s foremost expert on applied artificial intelligence and EY’s Entrepreneur of the Year in 2023, the internet is now a space where reliable information sits beside convincing fabrications, and no amount of earnest climate communication will fix this without tools that can separate accuracy from invention at scale.
AI is already showing what those tools might look like. It can review millions of words in seconds and test claims against established climate data with a consistency no human team can match. We are already seeing this in practice. For example, the machine-learning model ClimateBERT has analysed corporate reports and exposed misleading emissions claims. Another model, CLIMINATOR, has also been trained to hold political and corporate actors to account by checking whether their climate statements align with the evidence or contradict it. And the FactCrisis project, cofounded by the EU, has used AI during heatwaves to track false statistics and identify accounts pushing them, offering a glimpse of what becomes possible when AI and international bodies finally start reinforcing one another.
Duggal argues that the next step is a decentralized verification model. Climate data from satellites, sensors, and national inventories would sit in a shared public ledger that no ministry or corporation can quietly revise. When a government or company makes a claim about progress, anyone could check it against a record that does not bend to convenience. It would make the small acts of creative reporting that feed climate denialism far harder to get away with.
Yet today’s AI carries a flaw that limits its usefulness. Large language models are fluent but ungrounded, reproducing the language of climate science without retaining the facts that give it weight, which makes them unreliable referees in a space awash with motivated distortions. Duggal sees that any serious AI tool must reconnect claims to their evidence, trace where the data came from, and reveal the steps that turned information into a conclusion. This is the direction of his SeKondBrain project, which concentrates on how to build these evidential scaffolds so that an AI system can point to the exact documents, numbers, or assumptions that shaped its judgement. That kind of traceability matters because it gives climate negotiators and regulators something concrete to interrogate. And without systems built to preserve and expose the evidence behind their outputs, AI will remain too opaque to play any serious role in protecting science.
After the failures of COP29 and COP30, the process will only matter again if governments are finally pushed toward honesty and supported by tools that can hold them to it. Without that basic partnership, we may have reached the point where another COP has nothing left to say.
AI that monitors planetary health without a justice framework becomes sophisticated surveillance rather than equitable care.
Seven of nine planetary boundaries have been breached. Climate change, biosphere collapse, freshwater depletion and, for the first time, ocean acidification. These boundaries are the vital signs of a planet teetering beyond the range that sustained human civilization for 12,000 years. Alarm bells ring in every chart and graph of the Planetary Health Check 2025, yet our collective response remains inadequate.
Meanwhile, a technological revolution is underway. Artificial intelligence now processes vast satellite datasets to deliver near-real-time indicators of Earth's health. Initiatives from the Potsdam Institute and Stockholm Resilience Centre envision leveraging the latest satellite data and AI to create enhanced Earth monitoring systems, where machine-learning algorithms track carbon dioxide emissions, detect deforestation as it happens, and flag ecosystem stress long before human eyes register the crisis. AI promises faster, more precise environmental intelligence than ever before.
But there is a troubling blind spot in this approach. These powerful systems can quantify atmospheric CO2 down to decimal points, yet they cannot capture which communities suffer first when planetary boundaries break. They report that 22.6% of global land faces freshwater disturbance in streamflow, yet satellite dashboards remain silent on who lacks safe drinking water. They classify aerosol loading as within "safe" global limits even as monsoon disruptions devastate millions of farmers. Precise metrics obscure systemic inequities.
When aerosol pollution over South Asia weakens the monsoon—a lifeline for more than a billion people—satellites detect changing moisture indices but ignore caste-based water access, rural poverty, and entrenched social vulnerabilities that determine who drowns and who survives. Scholars warn of "computational asymmetries" and neocolonial dynamics in AI for climate action, perpetuating power imbalances by extracting information without empowering affected communities.
If AI-driven planetary monitoring is to fulfill its promise, it must be designed to protect everyone, especially the most.
Moreover, who controls these AI systems? Research centers in Europe and North America design and deploy them. Satellites are launched by NASA, the European Space Agency, and private firms. Datasets and codes are often proprietary. Access barriers exclude local researchers and grassroots organizations from meaningful participation. As a result, climate solutions driven by AI risk concentrating power in the same institutions that shaped the crisis rather than democratizing environmental protection.
This is not a call to reject AI in environmental science. On the contrary, these tools can transform early warning systems, improve emissions accounting, and optimize conservation strategies. The challenge lies in embedding justice at their core. We must ask urgent questions: Who has access to the data? Who shapes the algorithms? Who defines the metrics of success? AI that monitors planetary health without a justice framework becomes sophisticated surveillance rather than equitable care.
First, codesign monitoring systems with frontline communities. Indigenous Peoples, smallholder farmers, informal settlements—they possess critical local knowledge about changing environmental conditions. Participatory data collection initiatives, community-controlled sensor networks, and open-source platforms can bridge global datasets with ground truth.
Second, adopt data sovereignty principles. Data gathered from the Global South must remain accessible to local stakeholders. Intellectual property should not become a barrier to research and advocacy. Partnerships between Western labs and regional institutions must prioritize capacity building and fair data governance, following frameworks like CARE Principles for Indigenous Data Governance.
Third, expand AI metrics beyond biophysical variables. Incorporate indicators of social vulnerability—income inequality, water access, health outcomes—to contextualize environmental data. For example, freshwater disturbance indices should be mapped alongside demographic data on marginalized groups.
Finally, dedicate funding to interdisciplinary teams blending Earth system scientists, social scientists, and justice advocates. Building equitable AI systems requires collaboration across domains. Grant programs should support projects that integrate algorithm development with community engagement and policy analysis.
The machines watching our planet's vital signs can tell us when thresholds are crossed. They cannot tell us who pays the price. If AI-driven planetary monitoring is to fulfill its promise, it must be designed to protect everyone, especially the most vulnerable, rather than just refine our awareness of a crisis we're already failing to solve.
Here, justice must guide the next revolution in environmental intelligence.